
Hypertensive, obese with CHD
44 years old
 Case Presentation
Case Presentation
 Medical History
Medical History
 Questions
Questions
 Wrap Up
Wrap Up
CASE PRESENTATION
- The patient is now 44-years-old and weighs 119 kg
He visited the clinic with a BP of 180/130 mm Hg
He is complaining of gastric pain
The ECG showed
atrial fibrillation
mean heart rate was 142 bpm
frequent ventricular extra systoles
Depressed ST segment in inferior leads
He is unable to perform a treadmill test
You realize a stress echo showing inferior hypokinesia
An angiogram confirms stenosis of the second segment of the right CA, stented,
Return in sinus rhythm
MEDICAL HISTORY
- Diagnosis: Essential hypertension in obese patient with CHD
Obesity ,hypertension with atrial fibrillation revealing CAD
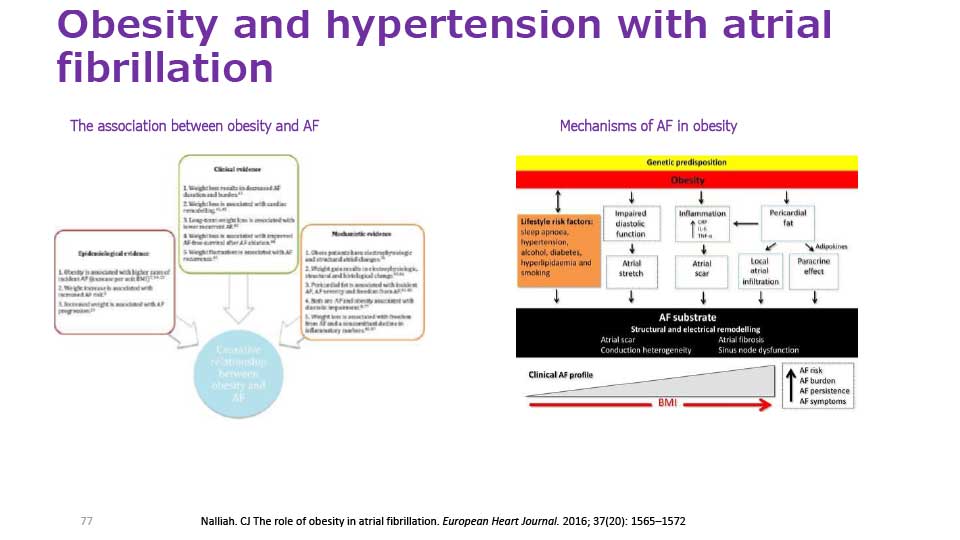
Obesity and hypertension with atrial fibrillation
{kind=link}
{kind=link}
QUESTIONS
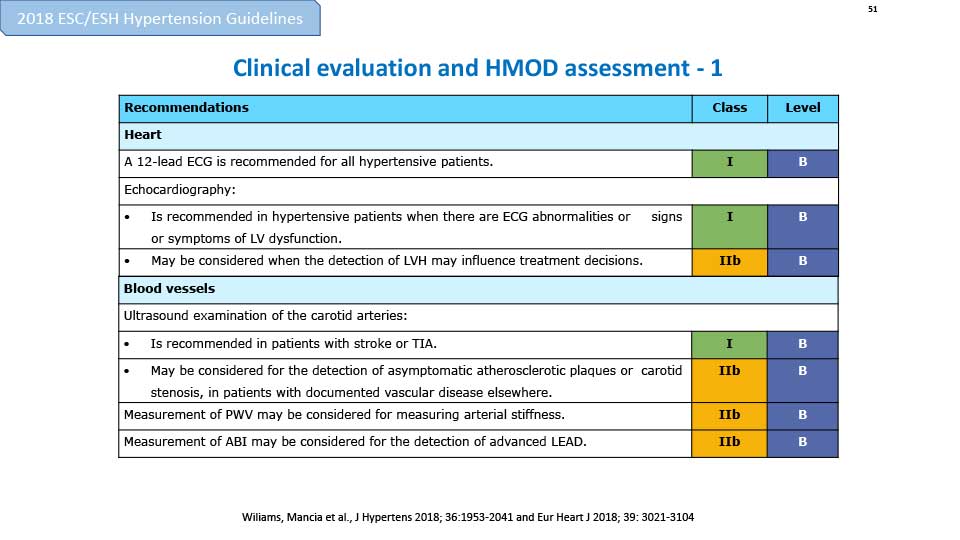
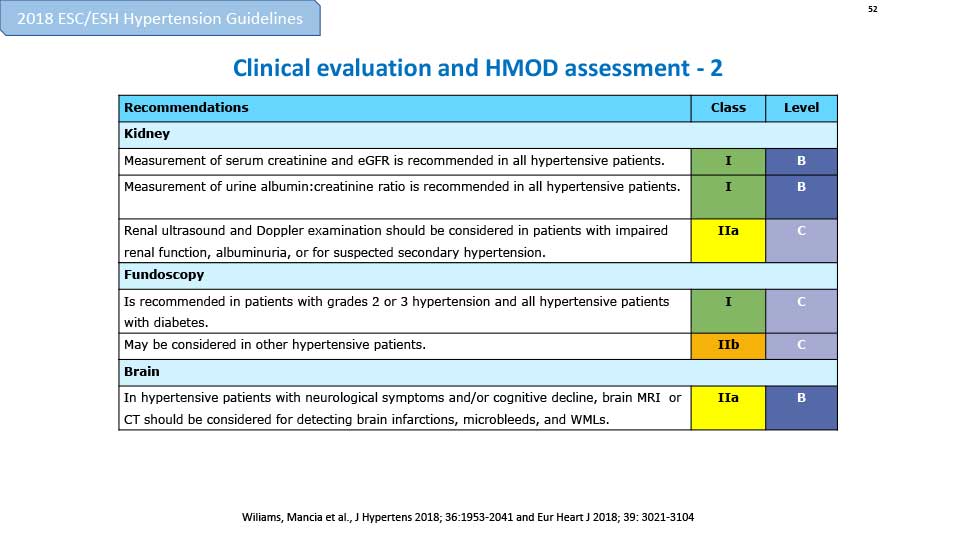
+ Do you think this is a case of hypertension-mediated organ damage.
- YES
- NO
{kind=link}
{kind=link}
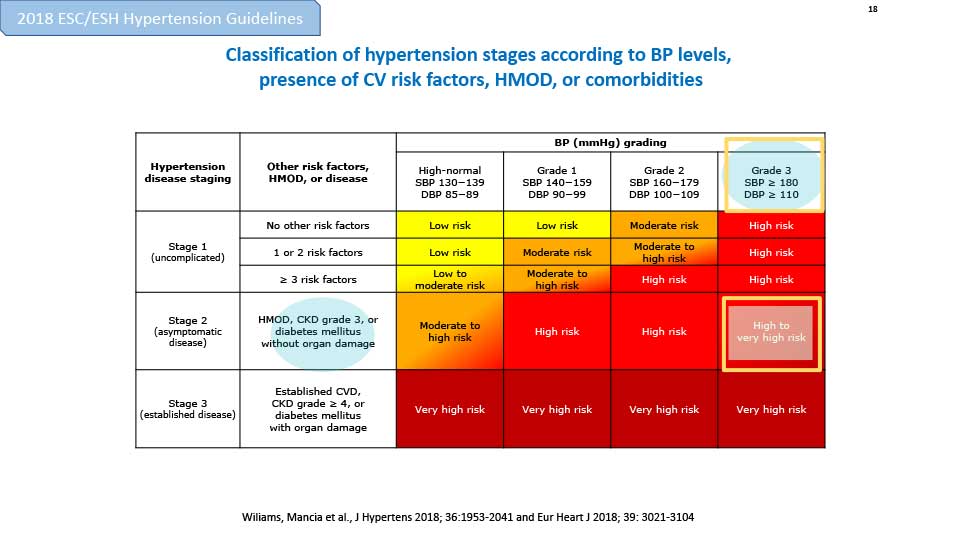
+ How would you classify HTN according to blood pressure levels, presence of cardiovascular risk factors, HMOD, or comorbidities?
Classification of hypertension stages according to BP levels, presence of CV risk factors, HMOD, or comorbidities
{kind=link}
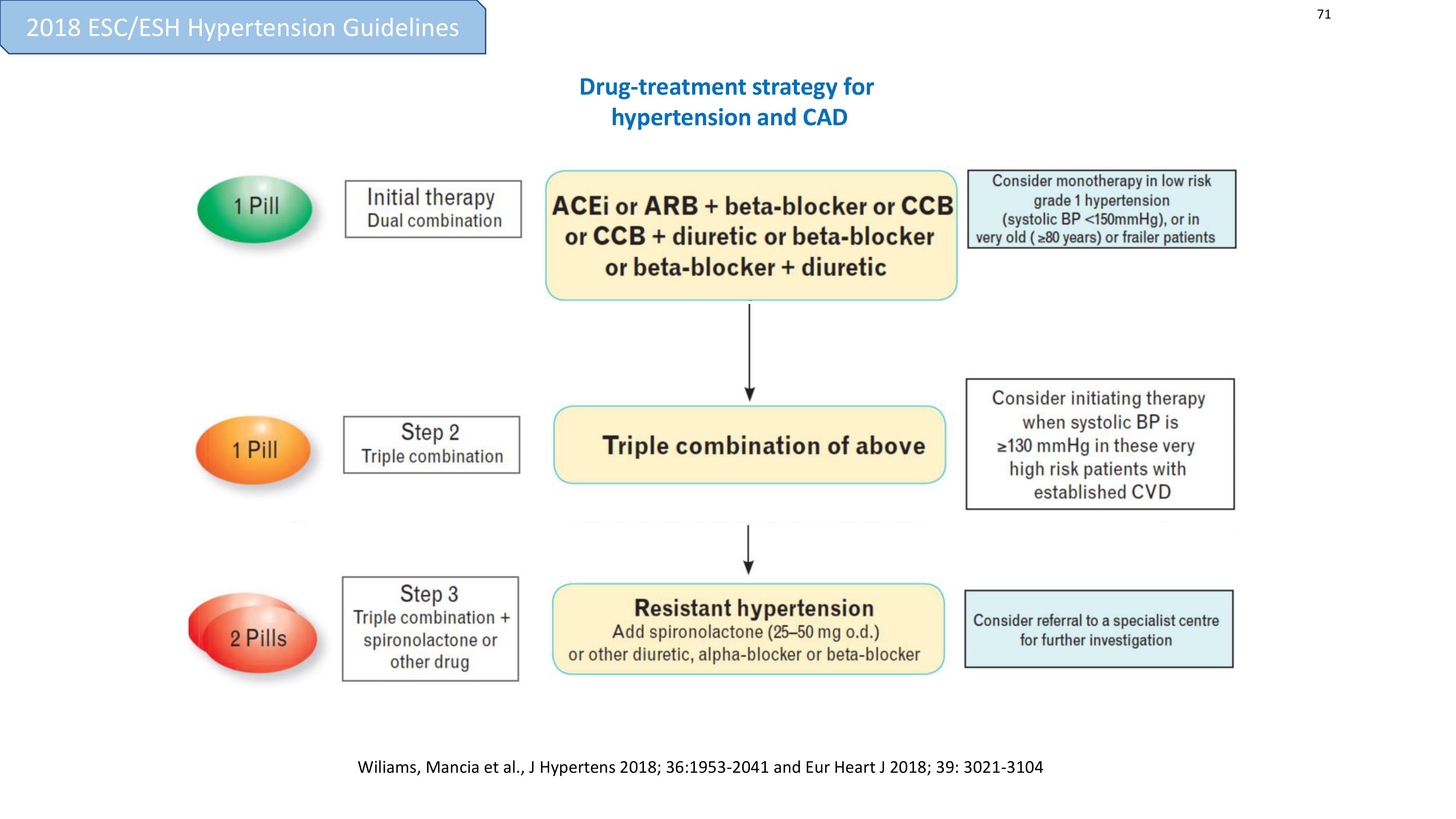
+ How should the case of HTN /atrial fibrillation/ CAD be treated?
- ACEi or ARB + CCB or diuretic
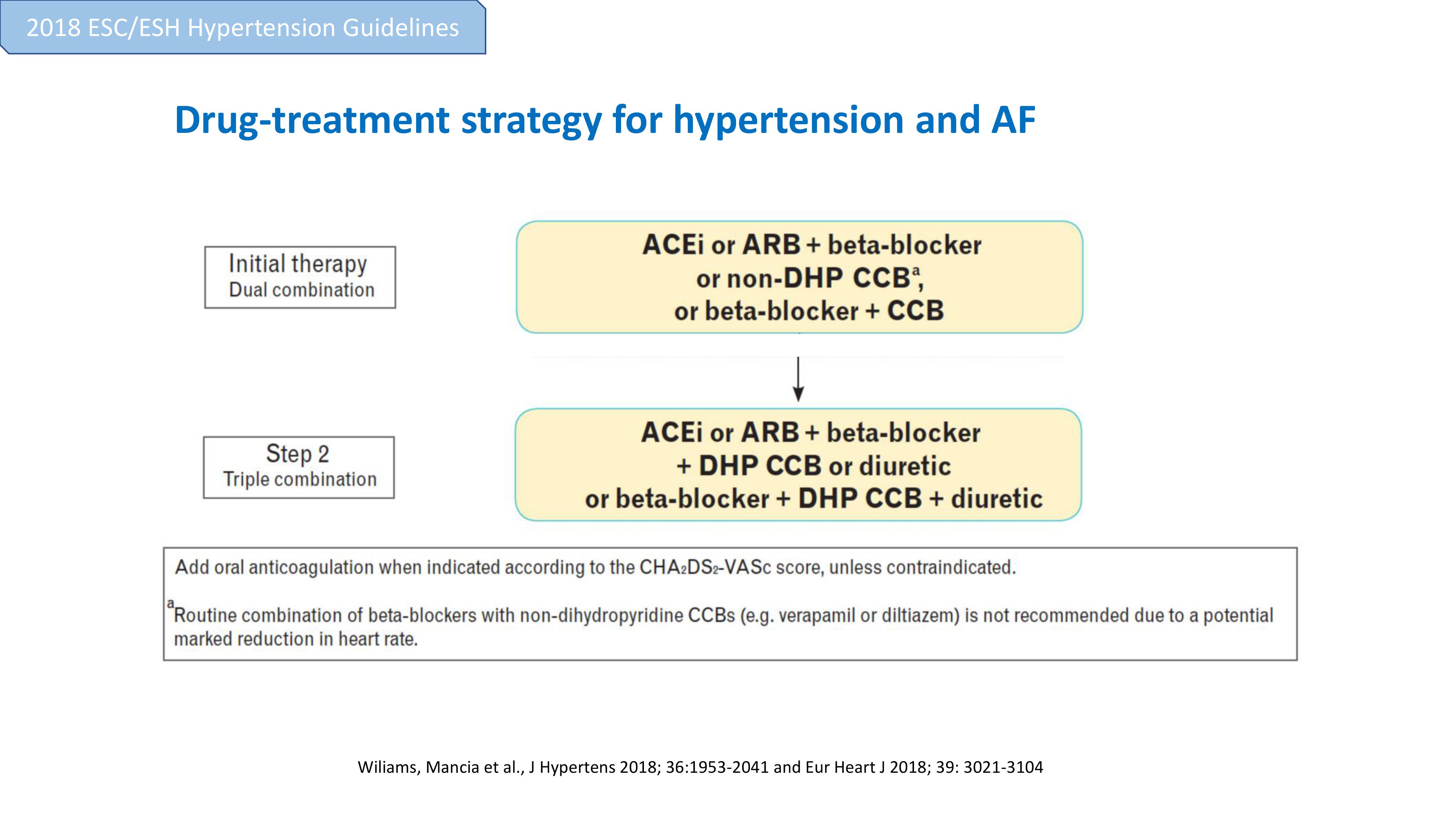
- ACEi or ARB + beta-blocker or CCB or CCB + diuretic or beta-blocker or beta-blocker + diuretic
- ACEi or ARB + CCB or ACEi or ARB + diuretic (or loop diuretic)
- ACEi or ARB + beta-blocker or non-DHP CCB, or beta blocker + CCB
Drug-treatment strategy for hypertension and CAD
{kind=link}
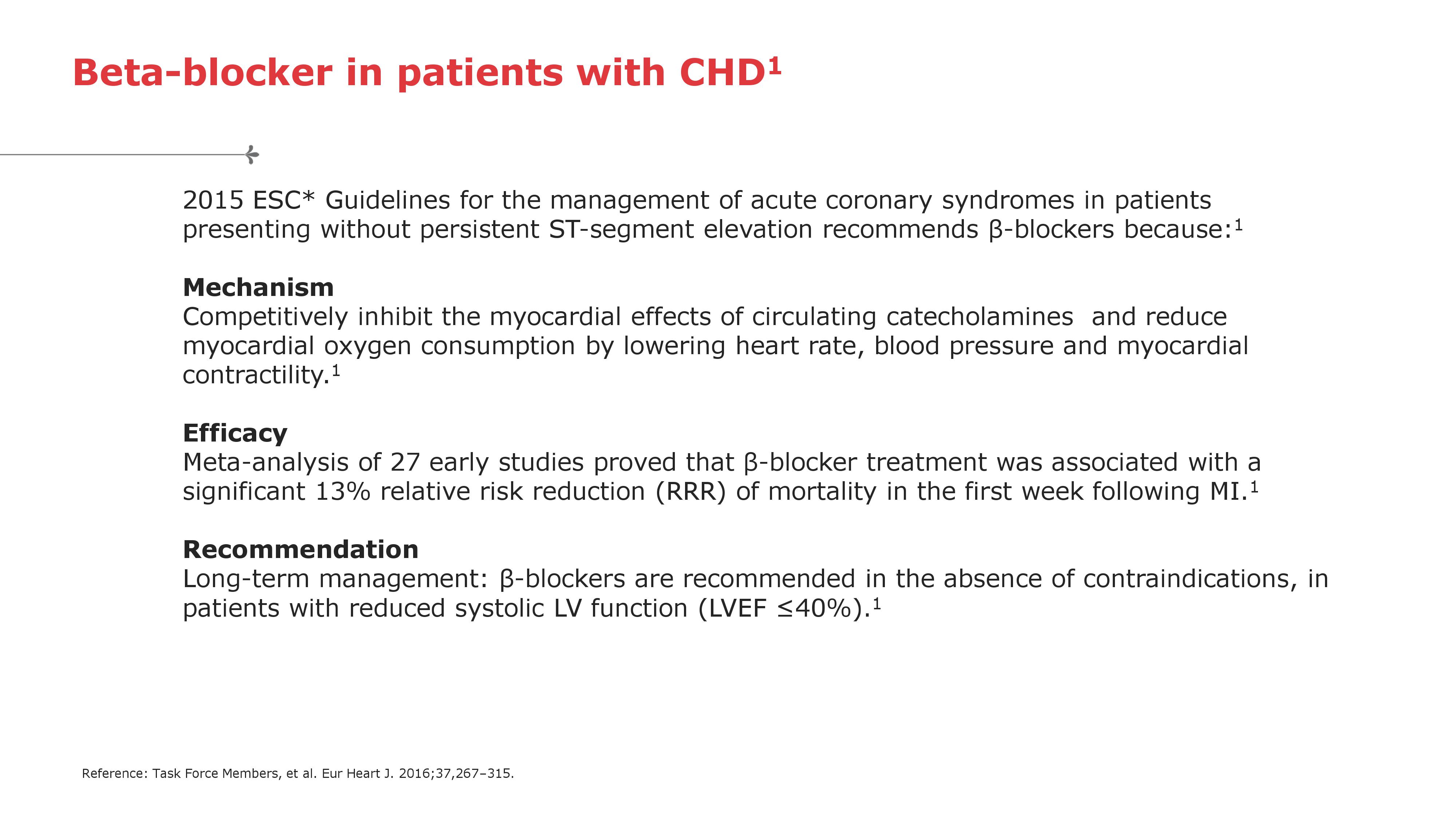
Beta-blocker in patients with CHD
{kind=link}
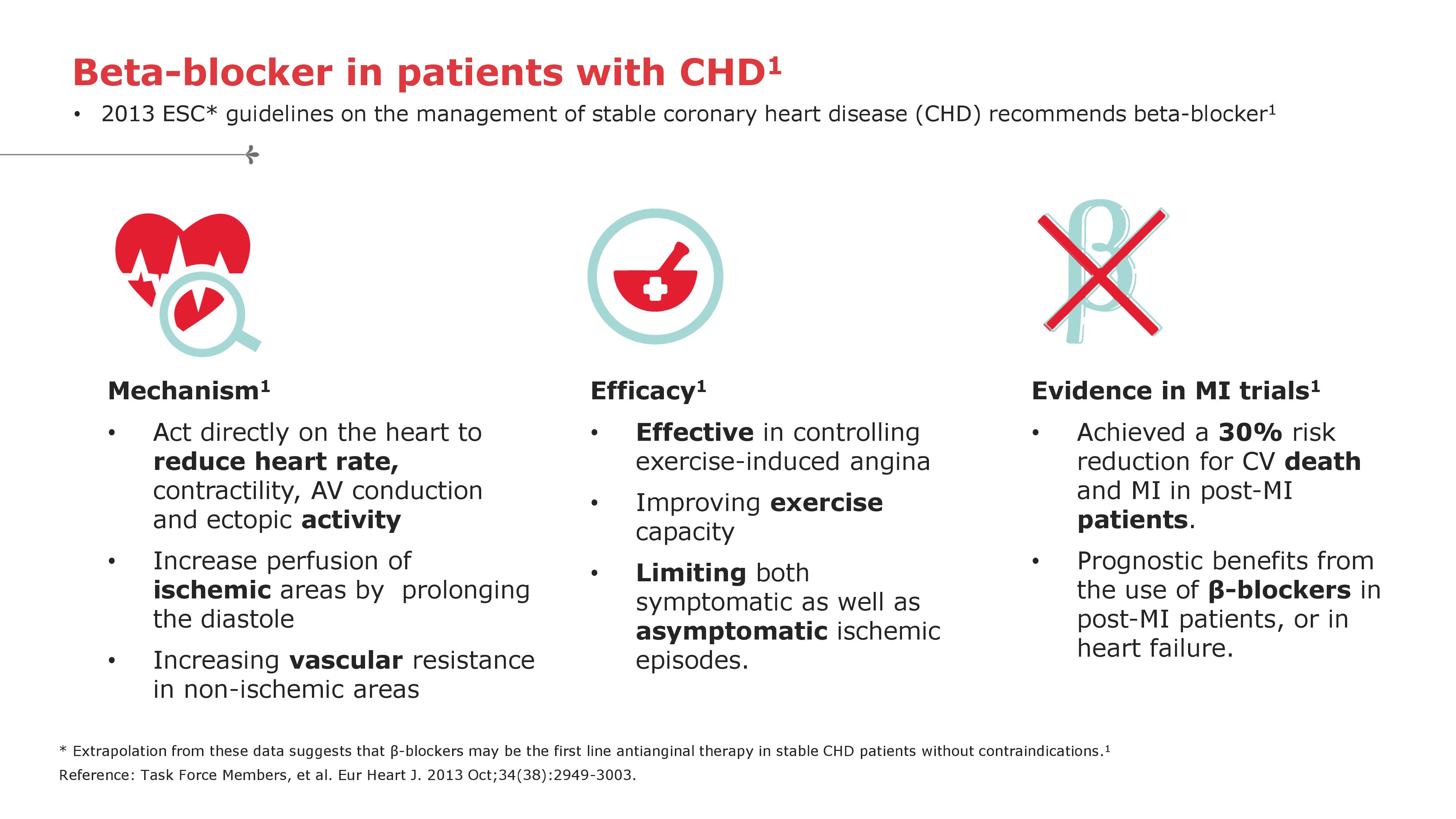
Beta-blocker in patients with CHD - 2
{kind=link}
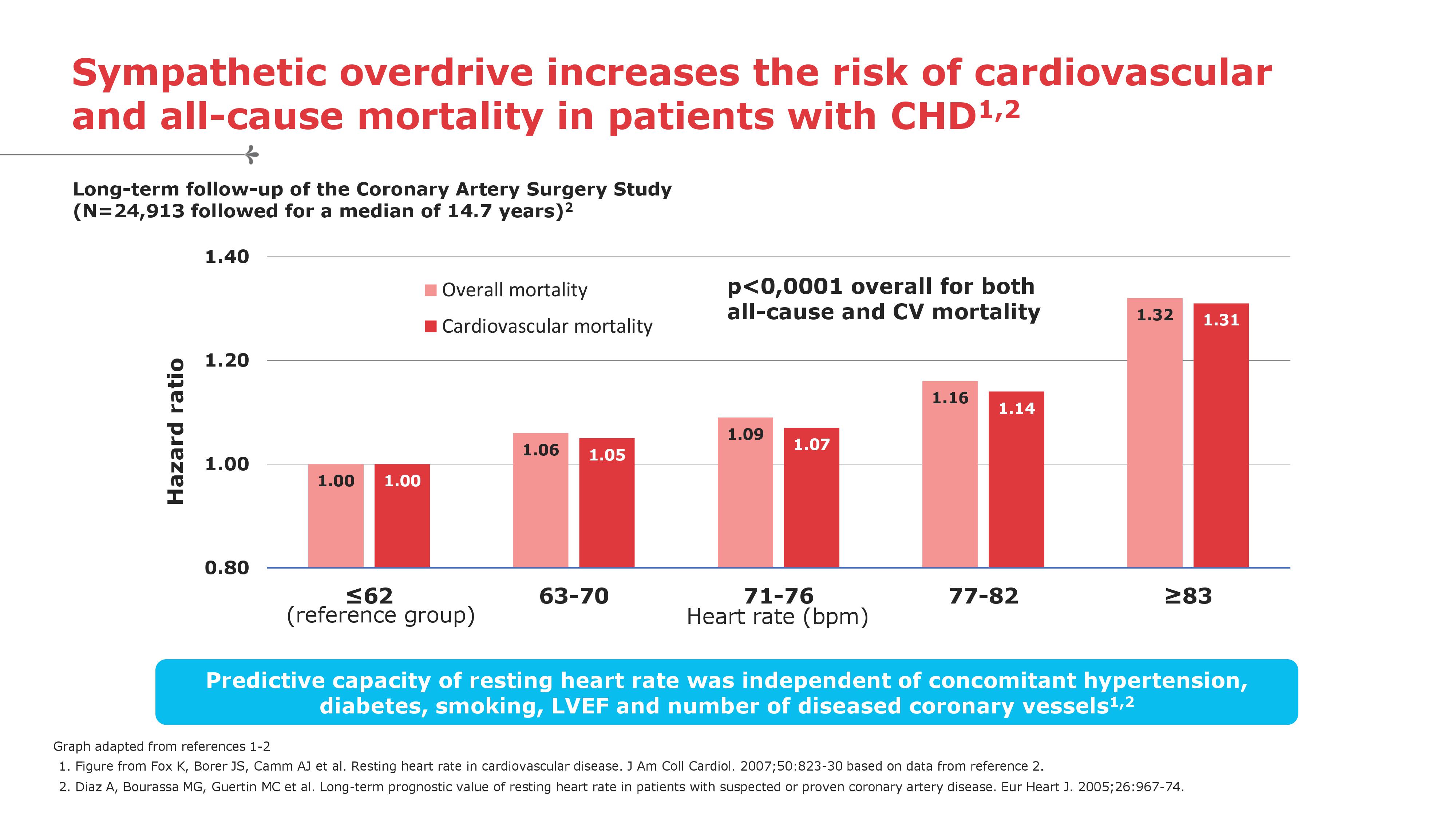
Sympathetic overdrive increases the risk of cardiovascular and all-cause mortality in patients with CHD
{kind=link}
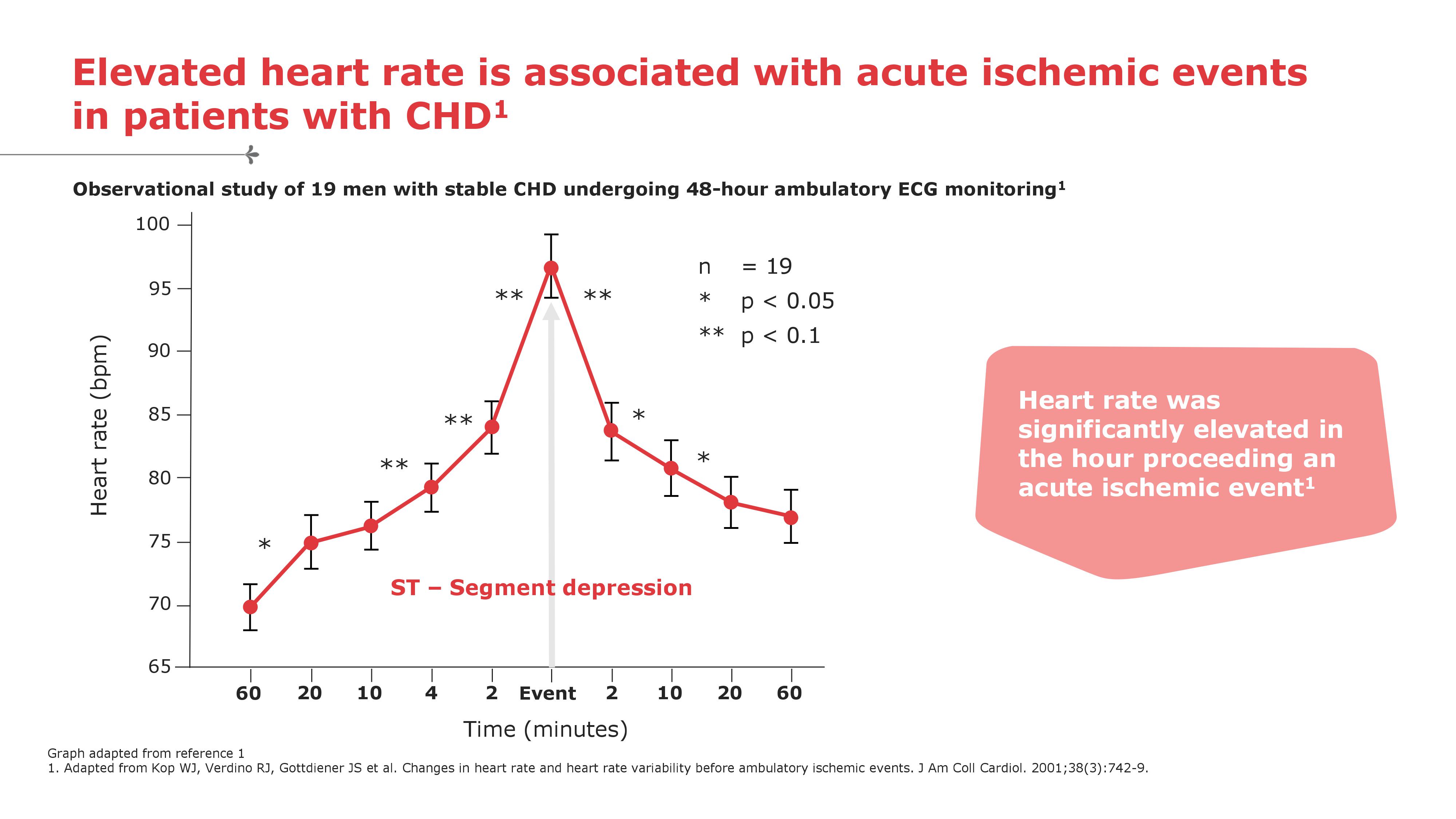
Elevated heart rate is associated with acute ischemic events in patients with CHD
{kind=link}
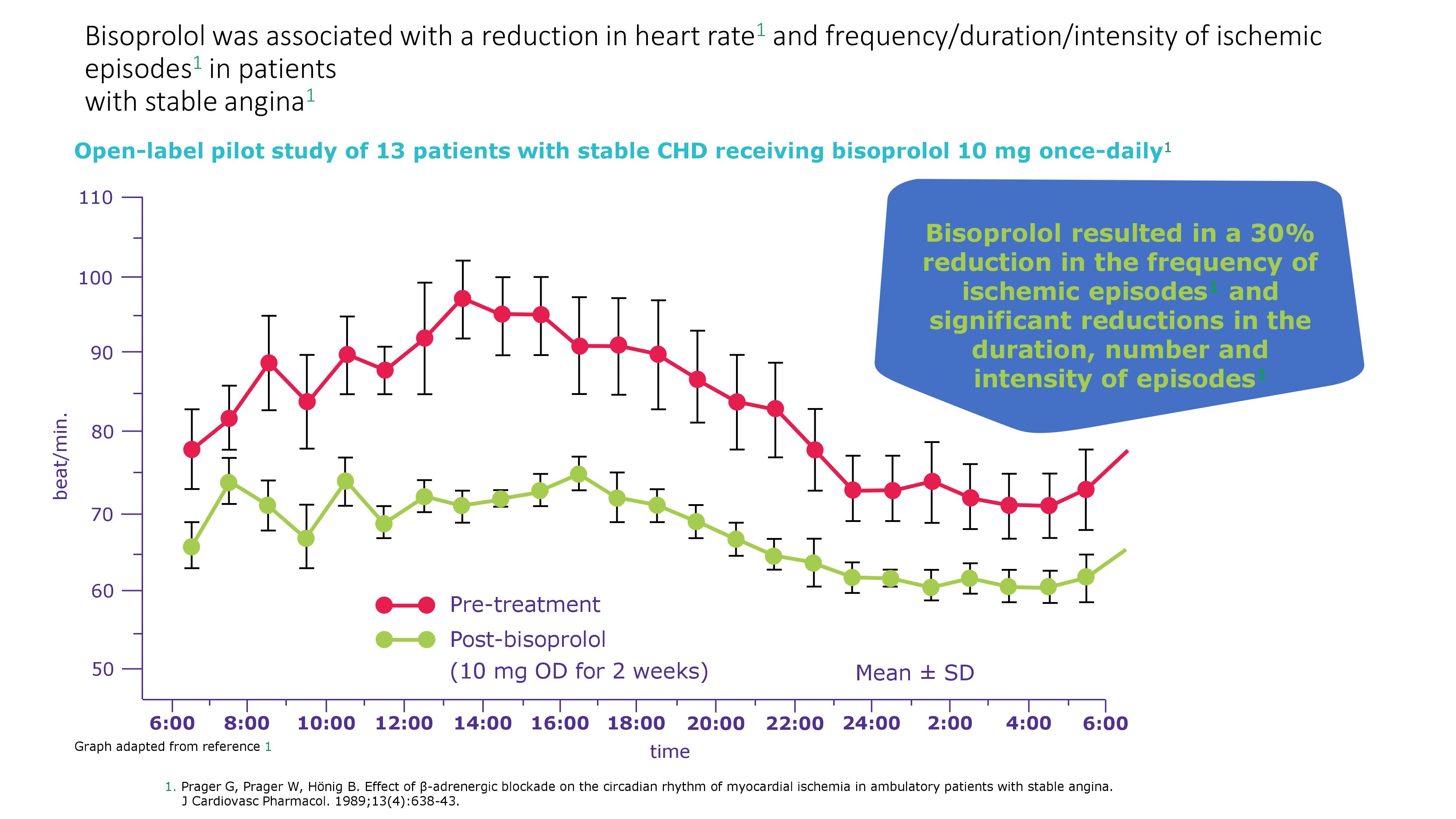
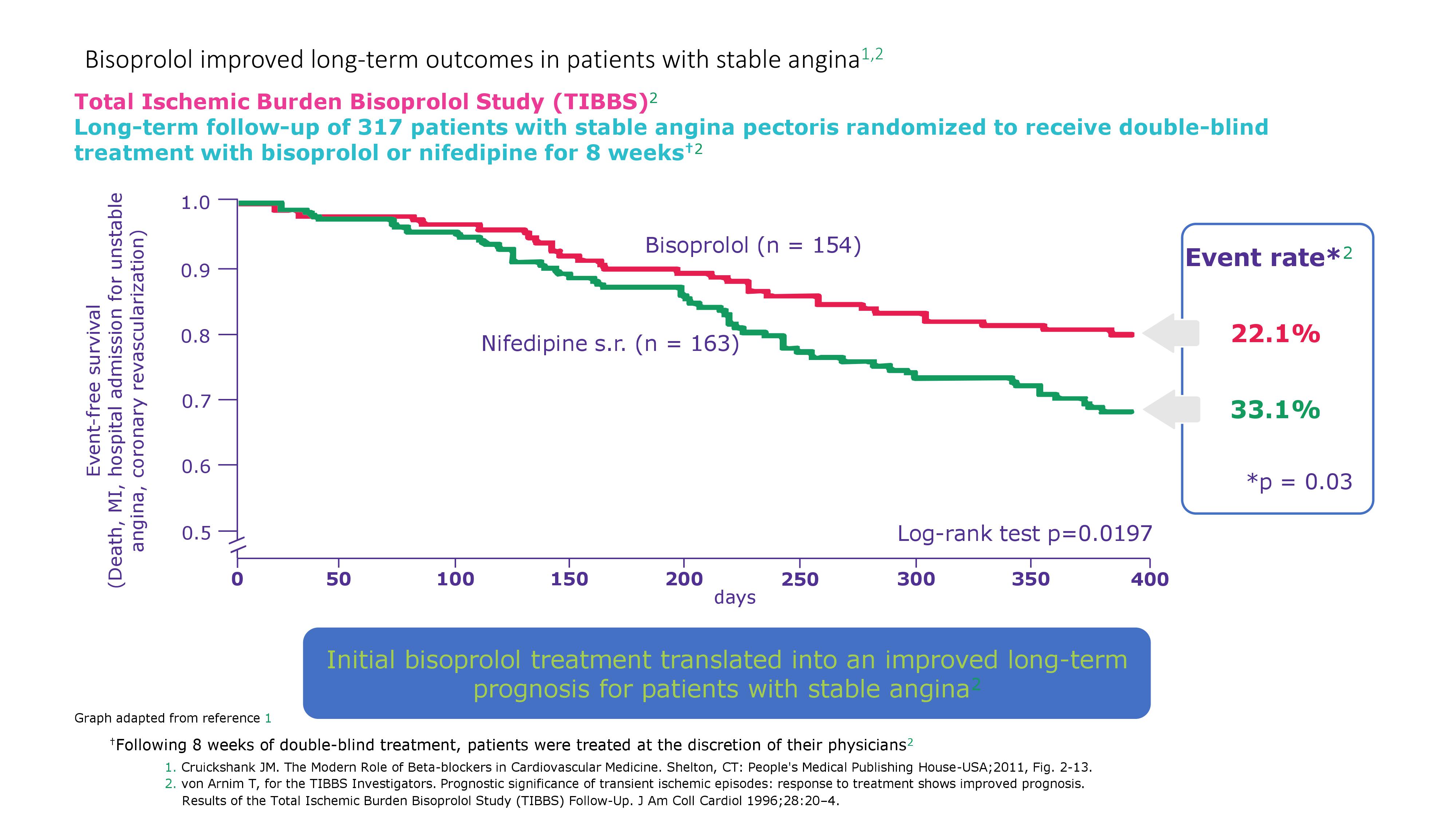
Bisoprolol was associated with a reduction in heart rate and frequency/duration/intensity of ischemic episodes in patients with stable angina
{kind=link}
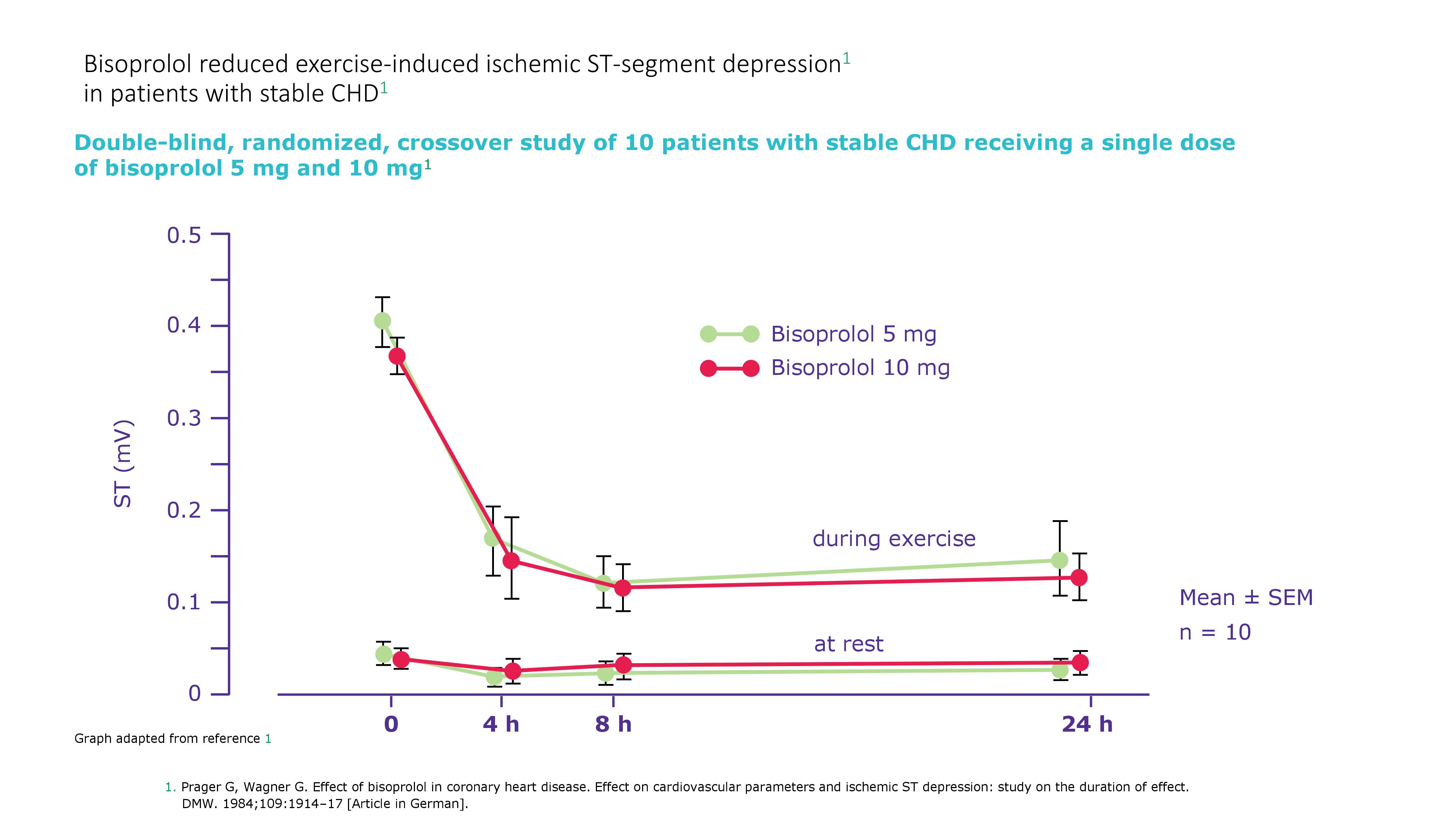
Bisoprolol reduced exercise-induced ischemic ST-segment depression in patients with stable CHD
{kind=link}
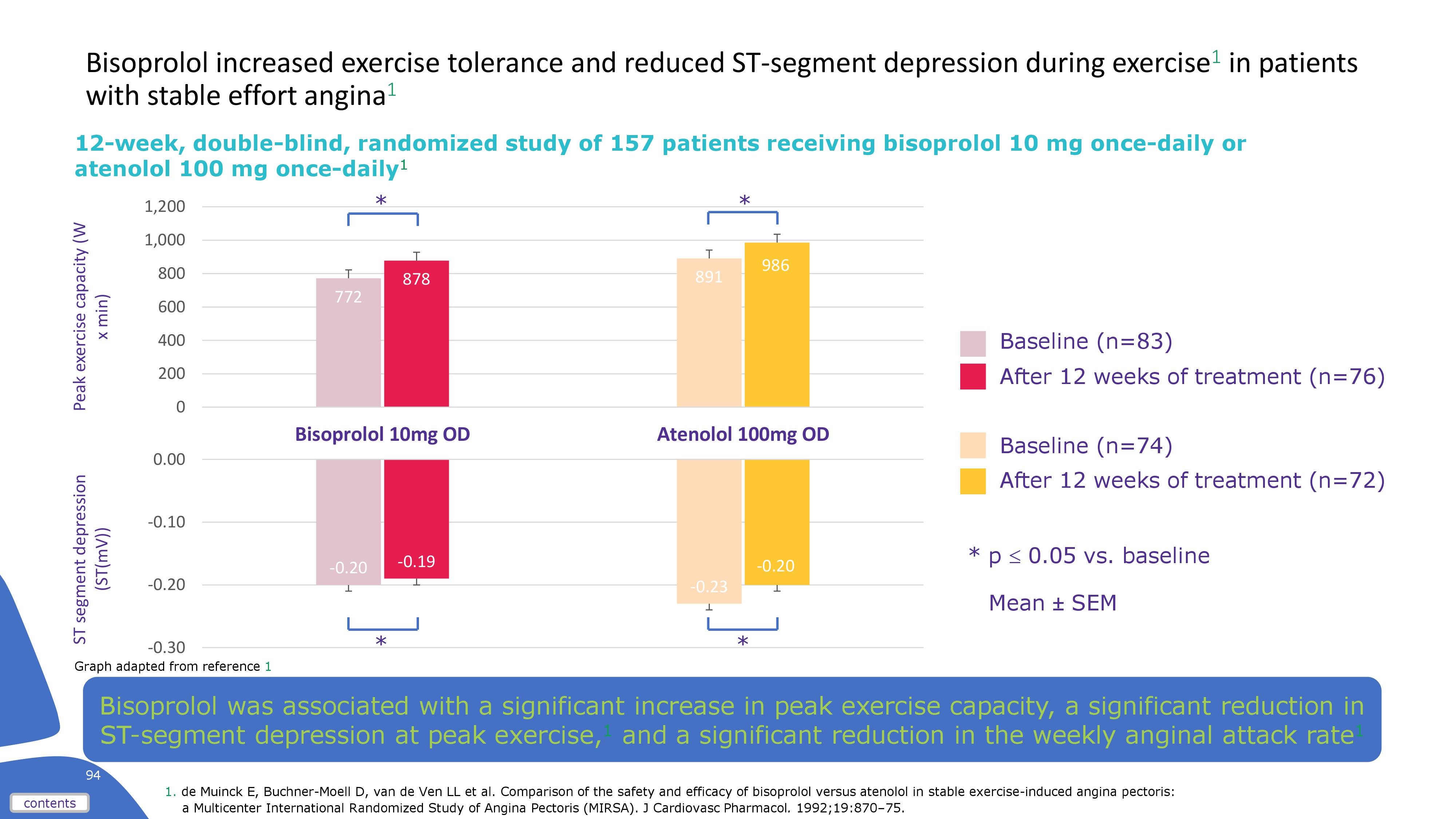
Bisoprolol increased exercise tolerance and reduced ST-segment depression during exercise in patients with stable effort angina
{kind=link}
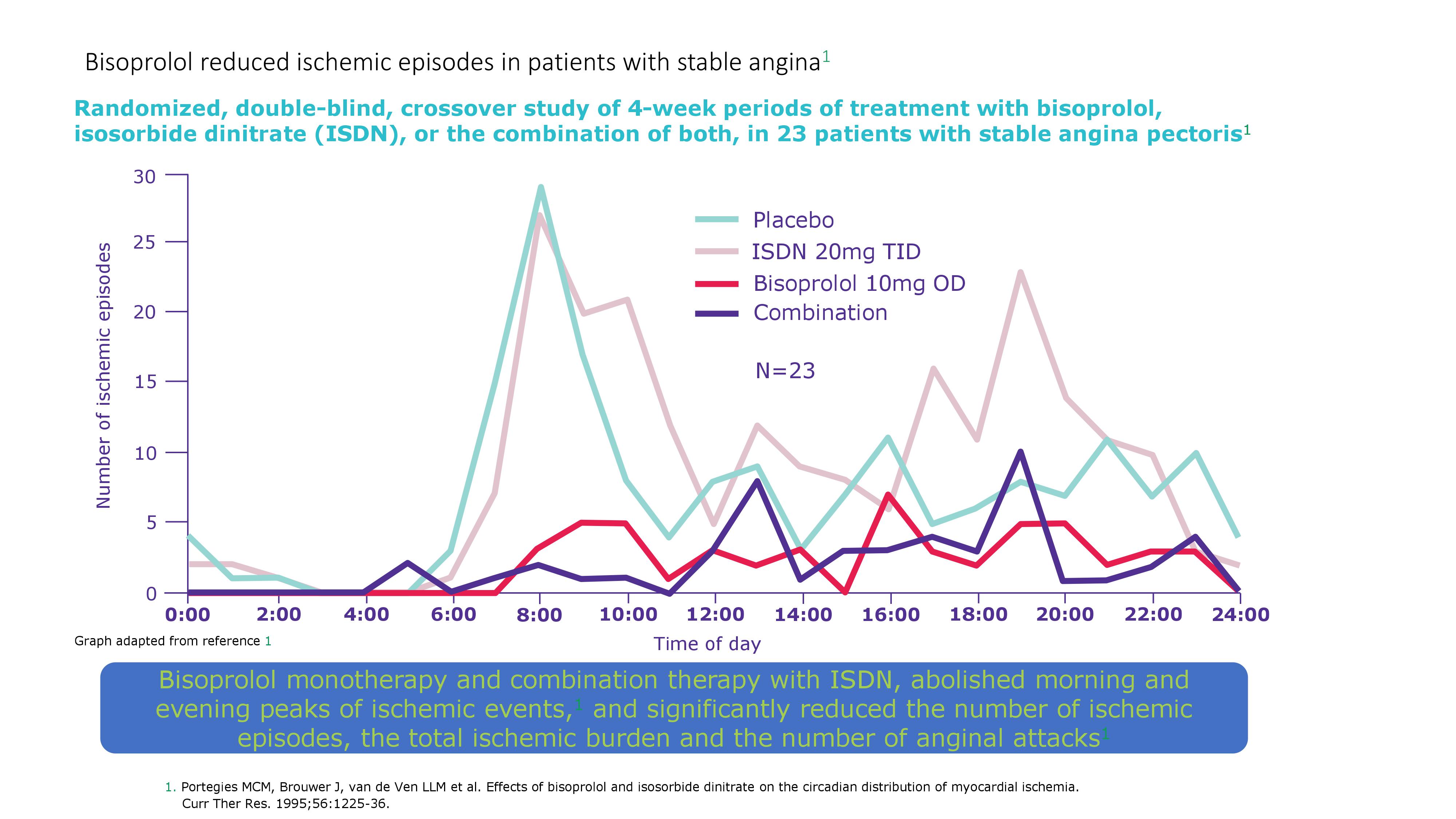
Bisoprolol reduced ischemic episodes in patients with stable angina - 1
{kind=link}
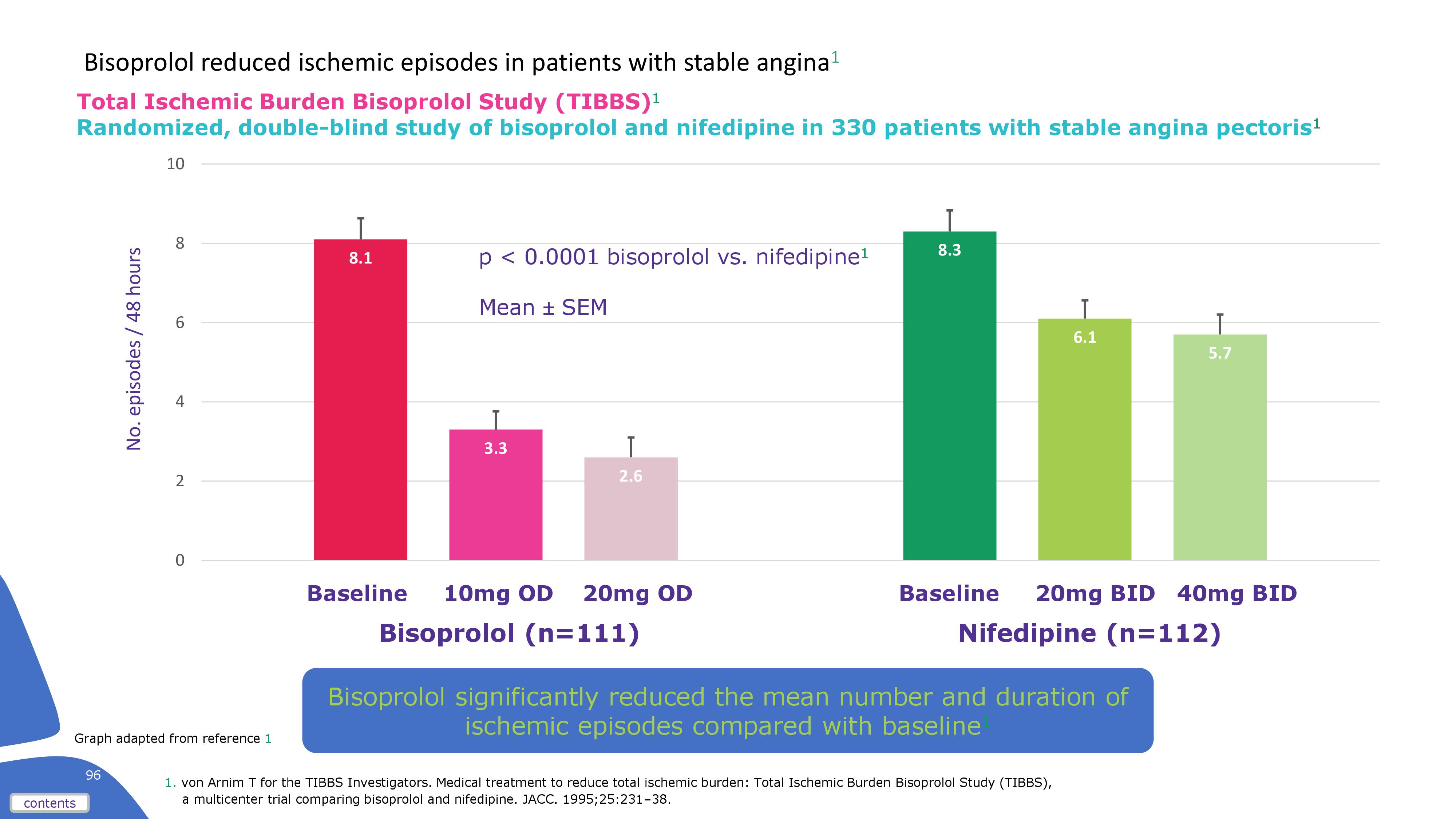
Bisoprolol reduced ischemic episodes in patients with stable angina - 2
{kind=link}
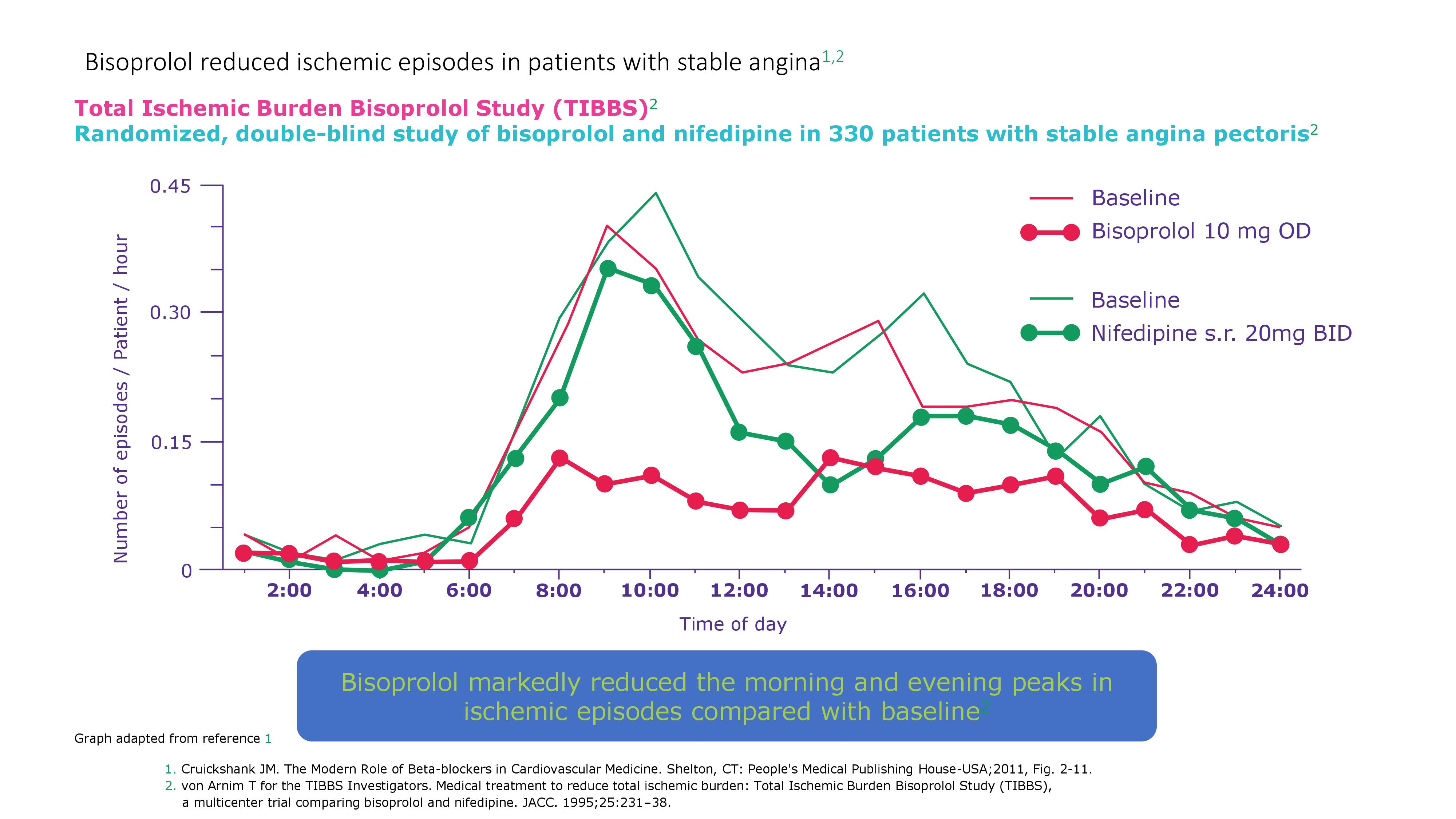
Bisoprolol reduced ischemic episodes in patients with stable angina - 3
{kind=link}
Bisoprolol reduced ischemic episodes in patients with stable angina - 4
{kind=link}
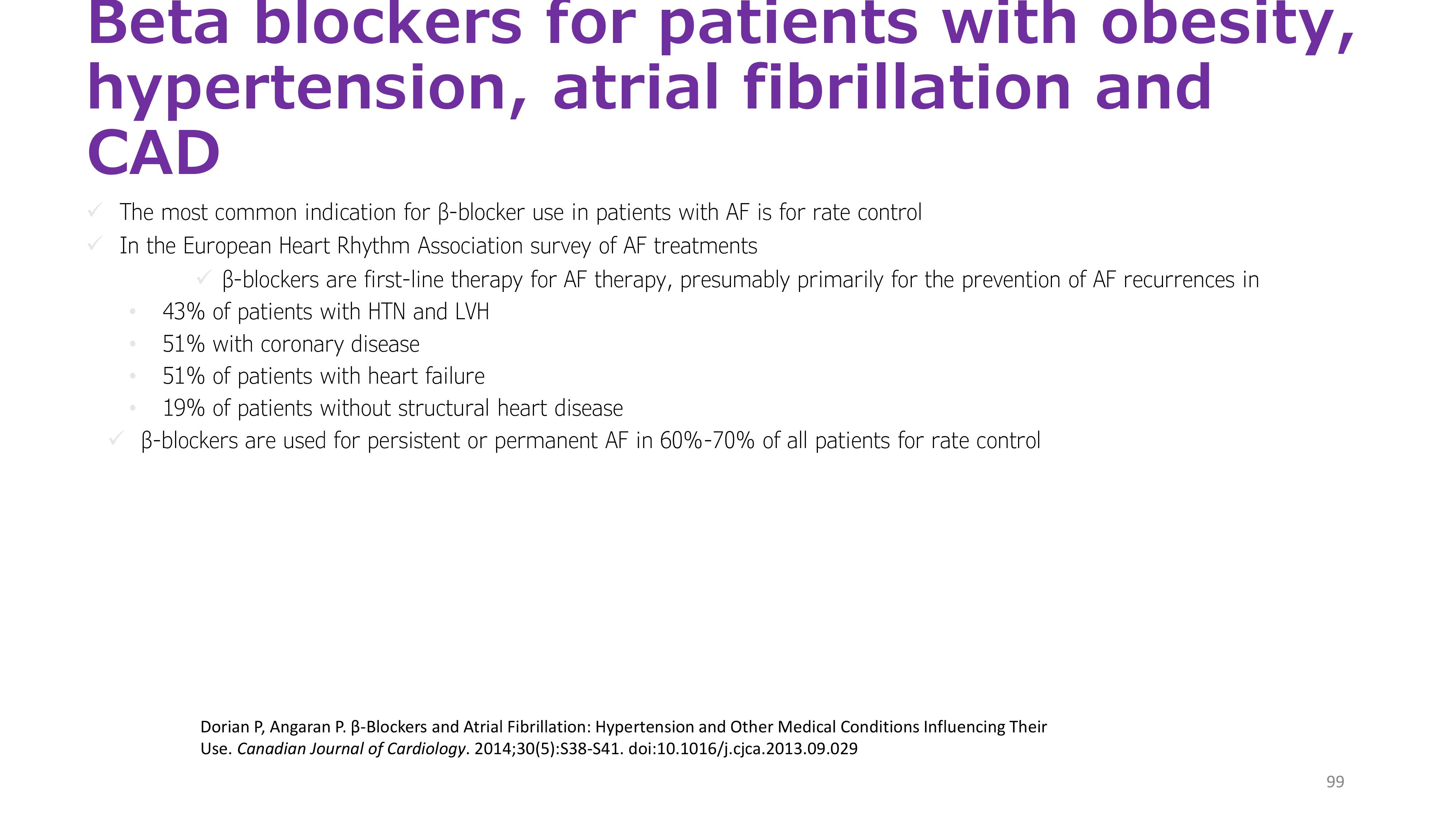
Beta blockers for patients with obesity, hypertension, atrial fibrillation and CAD
{kind=link}
Drug-treatment strategy for hypertension and AF
{kind=link}
+ Do you think Bisoprolol can be the choice of drug to treat a similar case?
- YES
- NO
EVIDENCE
Beta-blockers should be considered first line therapy to control the ventricular rate in patients with atrial fibrillation
They may also help to stabilize rhythm in patients with paroxysmal atrial fibrillation
They are preferred to Digoxin which is ineffective at limiting rate during exercise / sympathetic drive
Bisoprolol is the preferred oral therapy in patients with continuous atrial fibrillation
It is cardio-selective and offers good control of the ventricular rate
Starting dose is 2.5mg (1.25 mg in the elderly)
Bisoprolol exhibits a dose-responsive HR reduction when administered at sequential doses of 2.5 mg/day and 5 mg/day
Bisoprolol in heart rate reduction and in atrial fibrillation
Various β-blockers are used to control HR in AF; however, there have been few quantitative assessments of HR and blood pressure reductions with β-blocker monotherapy
A study by Yamashita T et al studied the effect of bisoprolol (2.5 mg/day) for 2 weeks in 78 patients with chronic (persistent or permanent) AF
48 patients judged to require a dose increase were either continued on 2.5 mg/day (24 patients) or administered a higher dose (5 mg/day; 24 patients) in a double-blind fashion for two further weeks
Change in mean HR as determined by Holter electrocardiogram was the primary endpoint
After 2 weeks of bisoprolol 2.5 mg/day, mean HR was significantly lower than that before treatment (12.2 ± 9.1 beats/min, p < 0.001)
Mean HRs in the 5-mg and 2.5-mg continuation groups were also significantly decreased compared with those before treatment (17.3 ± 12.9 and 11.4 ± 7.4 beats/min, respectively, both p < 0.001), with a significant between-group difference (p = 0.033)
The HR reduction was greater during the day than at night
Although a greater reduction in systolic blood pressure was seen in the 5-mg group than in the 2.5-mg continuation group, the difference between groups was not significant
There were no serious adverse events
WRAP UP
Objective:
The therapeutic approach should consider total CV risk in addition to BP levels in order to maximize cost-effectiveness of the management of hypertension.1
Efficacy
Greater SBP & DBP reduction vs. atenolol1, as well as other antihypertensive agents such as losartan, amlodipine and hydrochlorothiazide2 Better heart rate reduction vs. metoprolol,3 carvedilol and nebivolol4
β1-Selectivity
Bisoprolol is a third generation beta blocker with a remarkably high beta1-selectivity7
Safety profile
Minimal effects on blood glucose*, and lipids8-10, as well as lung function**8,11, peripheral circulation12-15, and male sexual function16
Consistent pharmacokinetic profile with a balanced renal clearance and hepatic metabolism17-19