
 Case Presentation
Case Presentation
 Medical History
Medical History
 Questions
Questions
 Case: Diagnosis
Case: Diagnosis
 Case: Treatment
Case: Treatment
 Wrap Up
Wrap Up
CASE PRESENTATION
- The patient, a 34-year-old man visited the clinic with complaints of frequent headaches, palpitations, and discomfort.
His office blood pressure measurement was 136/86 mm Hg.
ECG: Sinus Rhythm, Heart Rate 92 bpm.
Other than being overweight (106 kg; BMI=28.2 kg/m2), his examination was unremarkable.
A renal ultrasound showed normal-sized kidneys.
Doppler examination did not show renal artery stenosis.
His physician reassured him about the laboratory results and advised him to exercise.
MEDICAL HISTORY
- The patient was diagnosed with HTN when he was 22 years old, while in university.
He was then told that the elevated blood pressure was related to academic stress.
In the past, his BP levels were in range of 140-150 / 91-100-mm Hg and he weighed approximately 86 kg (body mass index [BMI] approximately 26.1 kg/m2).
He was not treated when he was diagnosed and was advised to change his lifestyle (i.e weight loss, exercice, low salt ..).
When he was 27 years old, he started working for a software start up.
He informed his physician that his mother and brother were known cases of HTN.
He was not aware of any history of strokes, kidney disease, endocrine tumors, or hypokalemia.
QUESTIONS
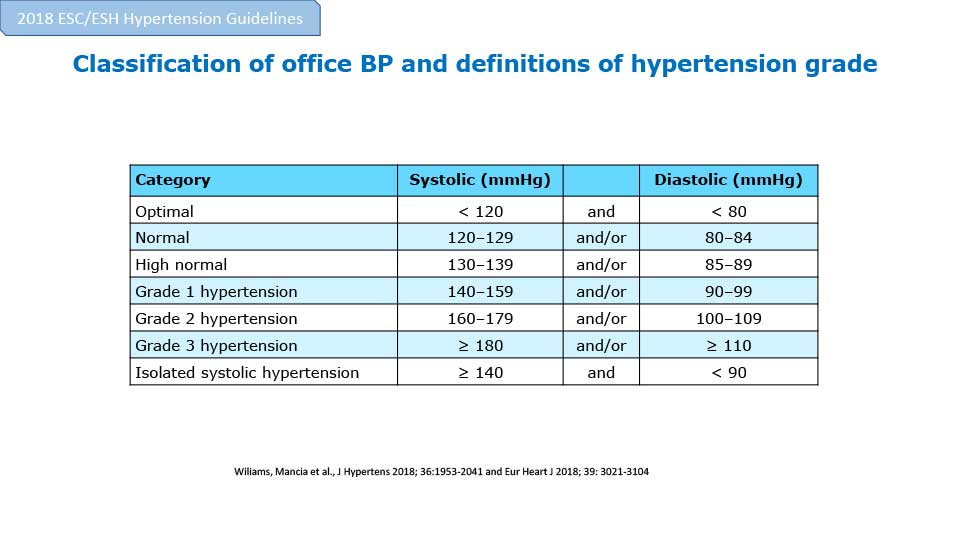
+ How will you classify office blood pressure in this case?
- Optimal
- Normal
- High normal
- Grade 1 hypertension
- Grade 2 hypertension
- Grade 3 hypertension
- Isolated systolic hypertension
{kind=link}
SHOW ANSWER
Patient’s systolic BP and diastolic BP fall under the category of high normal
+ How will you measure blood pressure?
- Office BP measurement
- Out of Office BP measurement
SHOW ANSWER
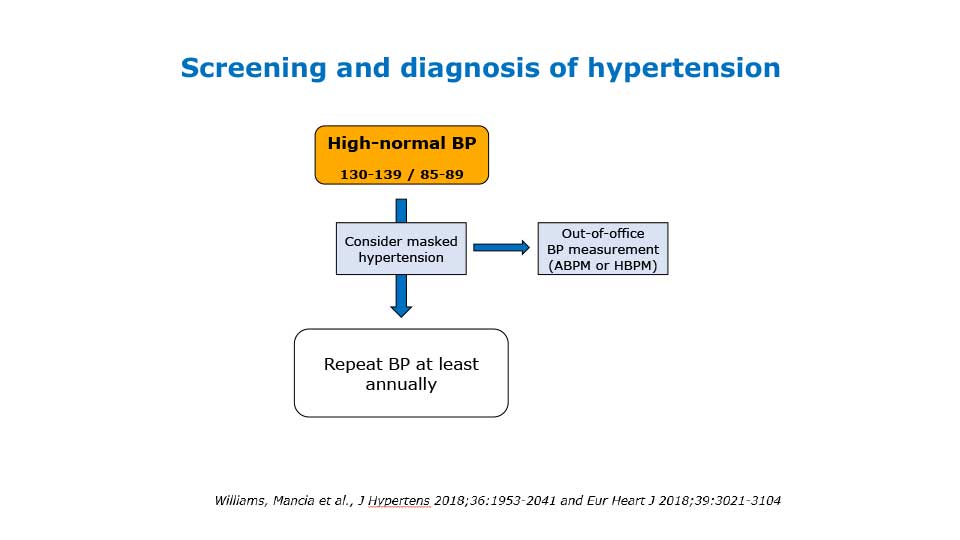
Ambulatory BP measurement /Home Blood Pressure Measurement
Evidence
The BP measurements done in the office may not reflect the home BP levels
Office BP may be elevated when the home BP is normal (white coat effect), or Office BP may be normal when the home BP is elevated (masked HTN)
Office measurements also do not reflect the diurnal variation and nocturnal BP levels
24 hours ambulatory BP monitoring (ABPM) is a precise method to quantify BP levels and diagnose HTN and inform about Heart Rate
ABPM may help to identify secondary HTN
Lack of nocturnal fall in BP may suggest the existence of sleep apnea
ABPM is particularly important for the management of HTN in diabetic patients, since HTN is a major risk factor for cardiovascular disease in these patients
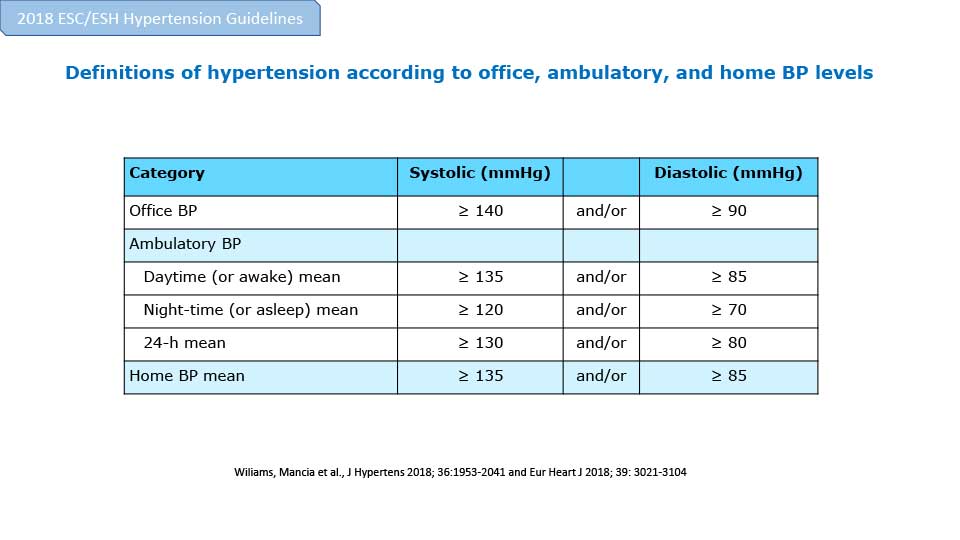
Screening and diagnosis of hypertension
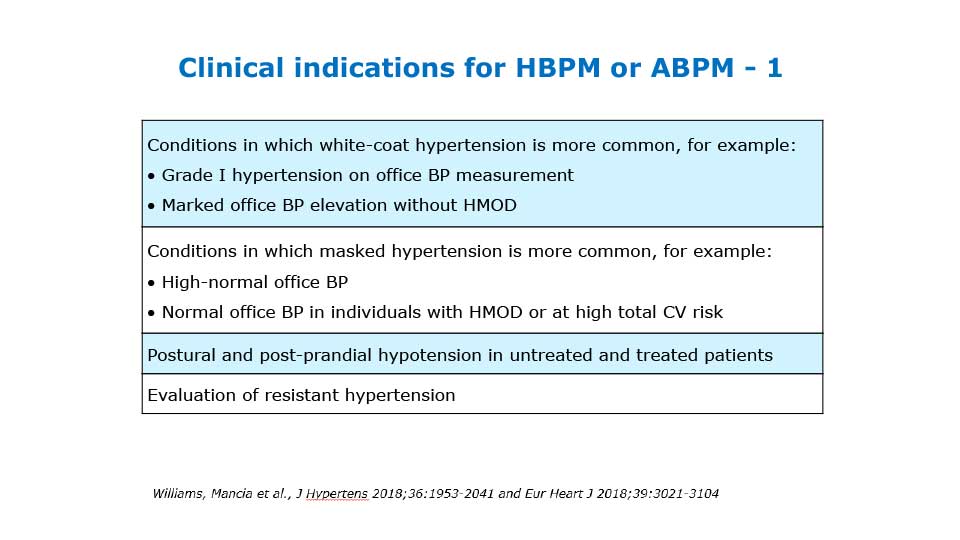
Clinical indications for HBPM or ABPM - 1
Evidence
The BP measurements done in the office may not reflect the home BP levels
Office BP may be elevated when the home BP is normal (white coat effect), or Office BP may be normal when the home BP is elevated (masked HTN)
Office measurements also do not reflect the diurnal variation and nocturnal BP levels
24 hours ambulatory BP monitoring (ABPM) is a precise method to quantify BP levels and diagnose HTN and inform about Heart Rate
ABPM may help to identify secondary HTN
Lack of nocturnal fall in BP may suggest the existence of sleep apnea
ABPM is particularly important for the management of HTN in diabetic patients, since HTN is a major risk factor for cardiovascular disease in these patients
Screening and diagnosis of hypertension
{kind=link}
Clinical indications for HBPM or ABPM - 1
{kind=link}
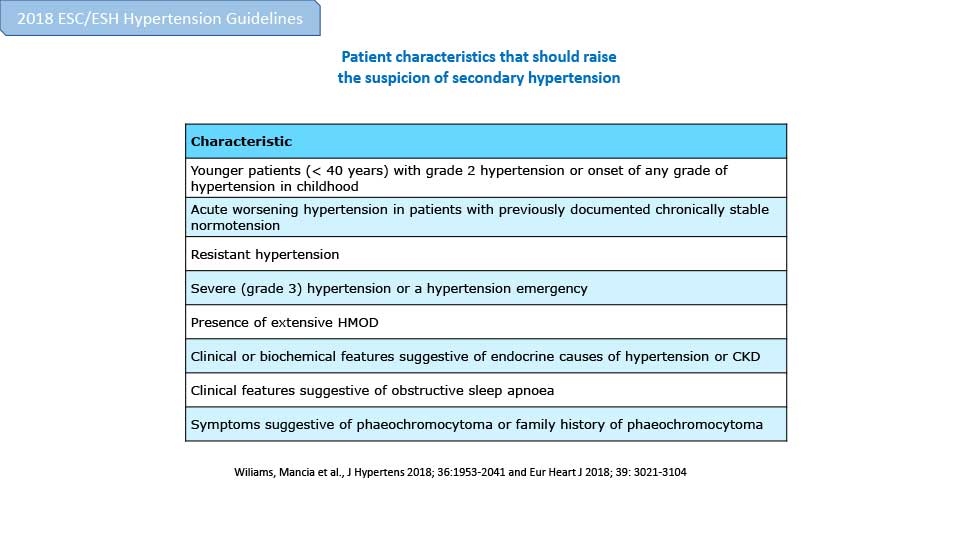
+ How will you exclude the secondary causes of hypertension?
- Rule out the use of hypertensogenic substances
- Assess some features to exclude secondary causes
{kind=link}
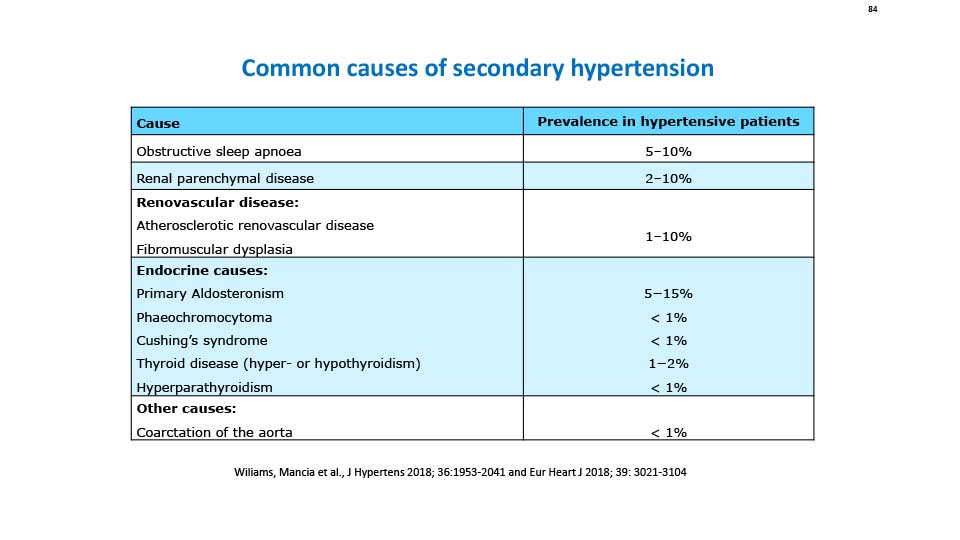
+ What are the causes of secondary HTN that have to be excluded?
- Renal parenchymal disease (e.g. glomerulonephritis)
- Renovascular disease (e.g. renal artery stenosis)
- Mineralocorticoid-mediated hypertension (e.g. primary hyperaldosteronism)
- Catecholamine-mediated hypertension (e.g. phaeochromocytomas)
- Medication (e.g. the oral contraceptive pill)
- Abuse of cocaine or amphetamines
SHOW ANSWER
All of the above and more specific age- related cause
Common causes of secondary hypertension
Common causes of secondary hypertension
{kind=link}
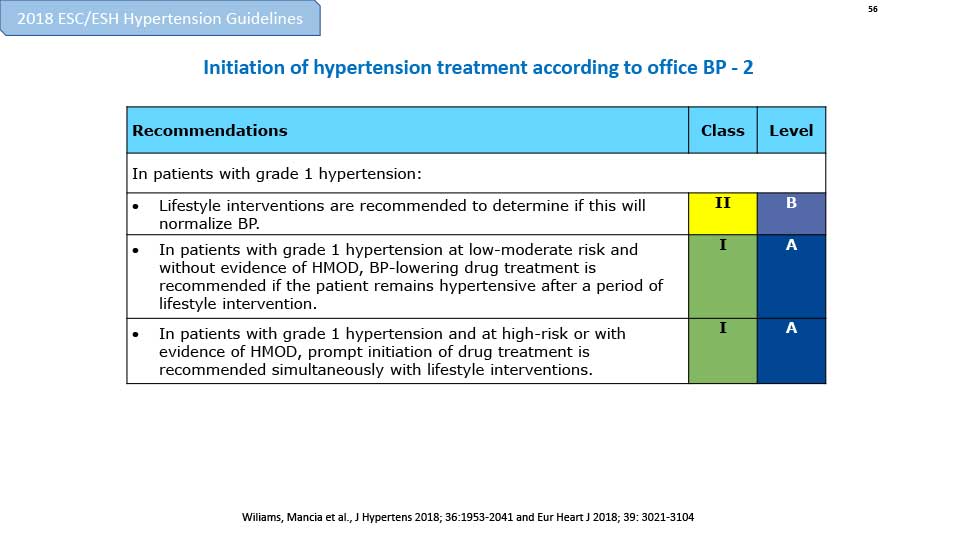
+ Considering the diagnosis, how would you treat the patient?
- Lifestyle modification
- Start him on a BB
- Start him on a CCB
- Start him on a diuretic
- Start him on a RAS blocker
- Start him on another antihypertensive agent
2. Williams B et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal. 2018. 39(33); 3021–3104
SHOW ANSWER
Lifestyle modification
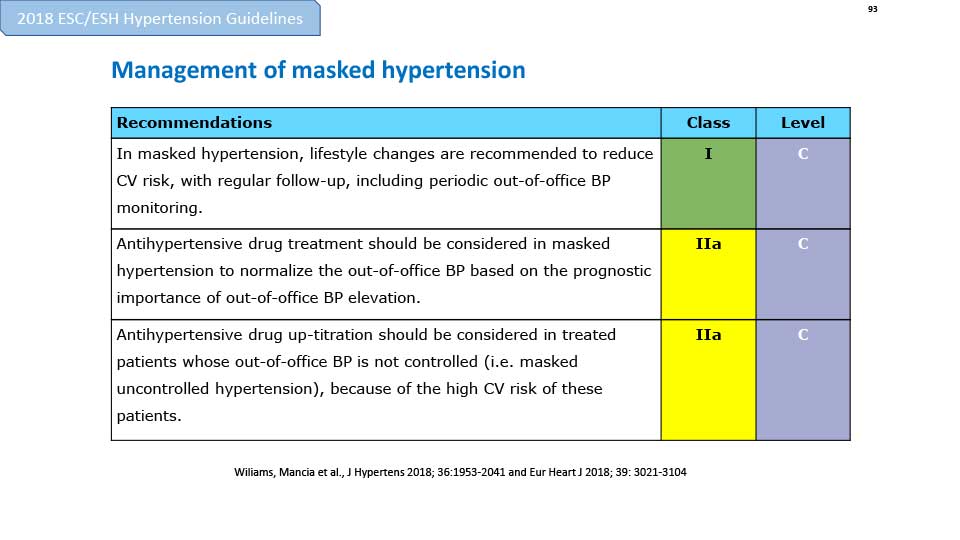
Start an antihypertensive agent
Management of masked hypertension
Initiation of hypertension treatment according to office BP - 2
Start an antihypertensive agent
Management of masked hypertension
{kind=link}
Initiation of hypertension treatment according to office BP - 2
{kind=link}
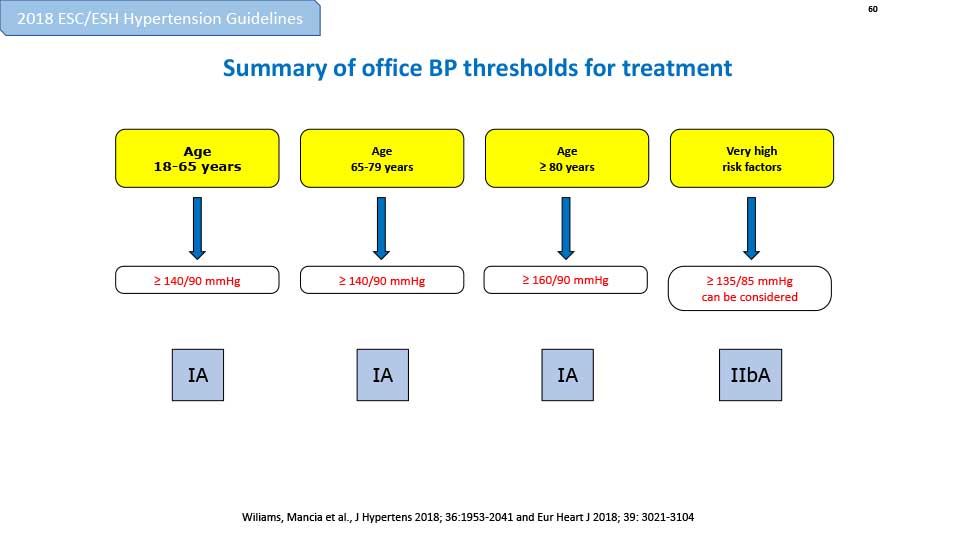
+ What should be the BP threshold for treatment in such a case?
- SBP≥140, DBP≥90
- SBP≥90, DBP≥90
- SBP≥140, DBP=90
SHOW ANSWER
SBP≥140, DBP≥90
Summary of office BP thresholds for treatment
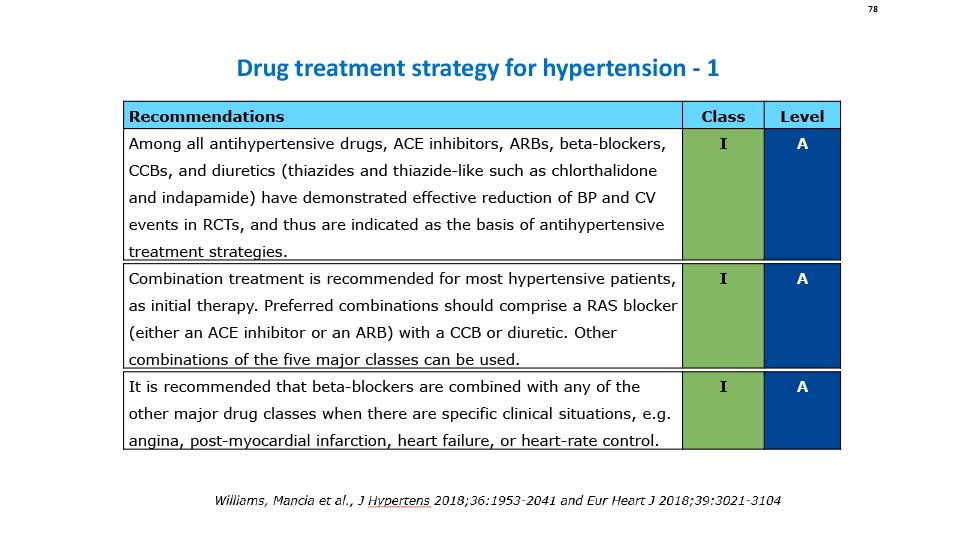
Drug treatment strategy for hypertension - 1
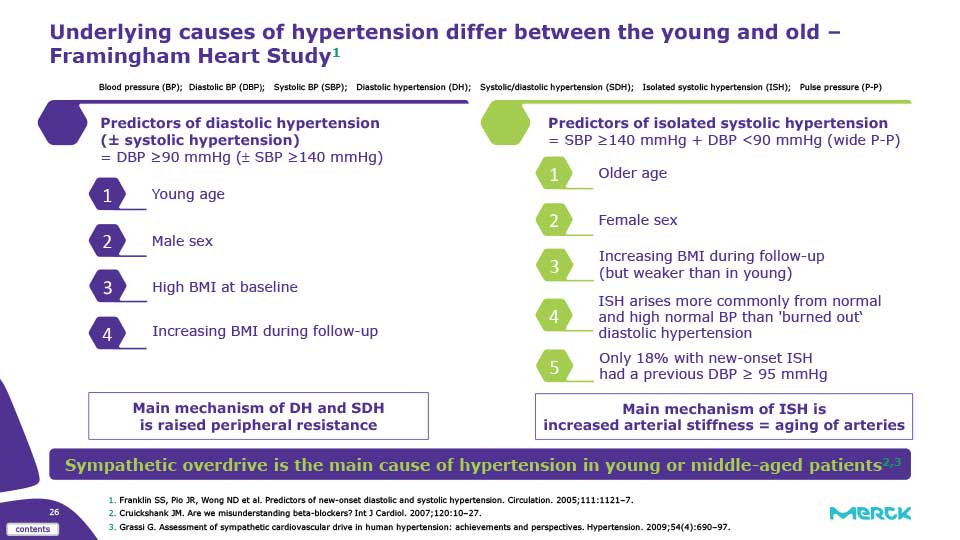
Underlying causes of hypertension differ between the young and old – Framingham Heart Study
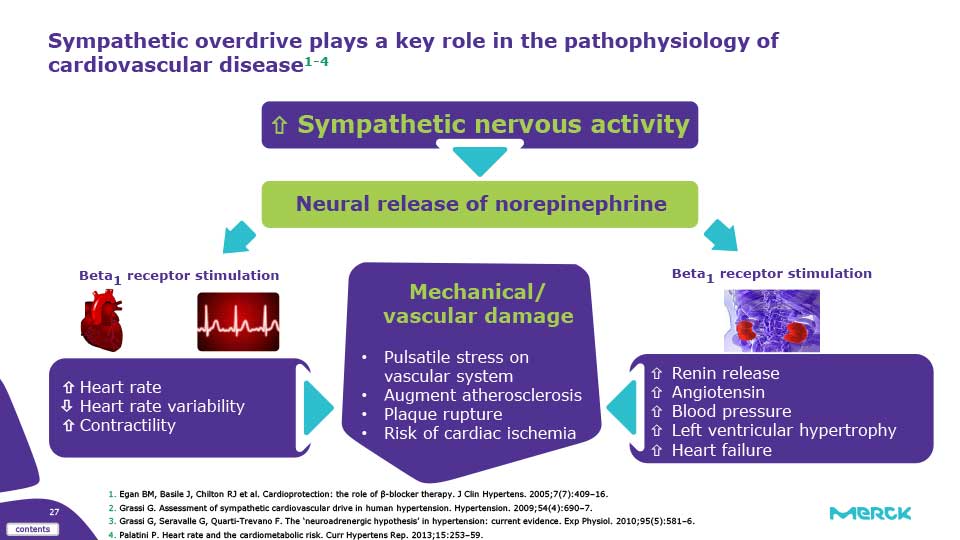
Sympathetic overdrive plays a key role in the pathophysiology of cardiovascular disease
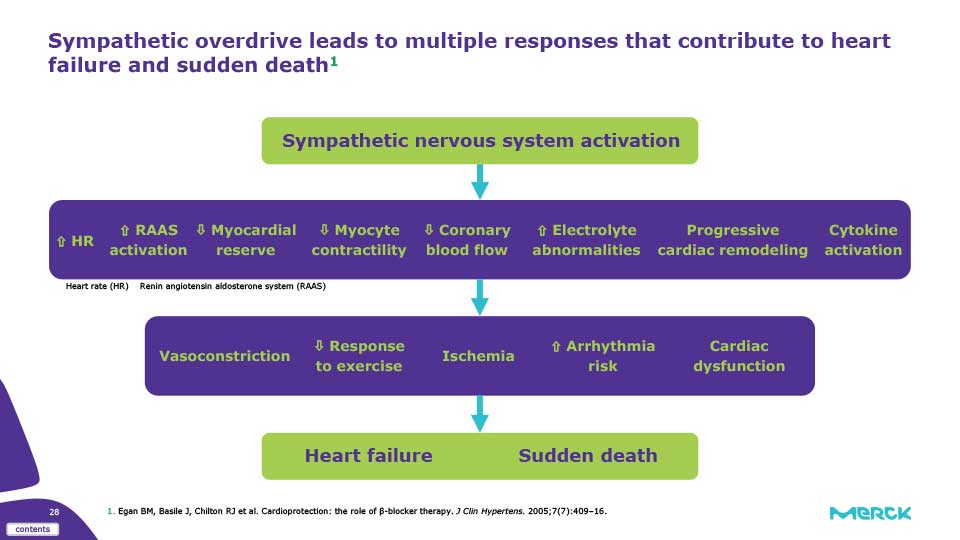
Sympathetic overdrive leads to multiple responses that contribute to heart failure and sudden death
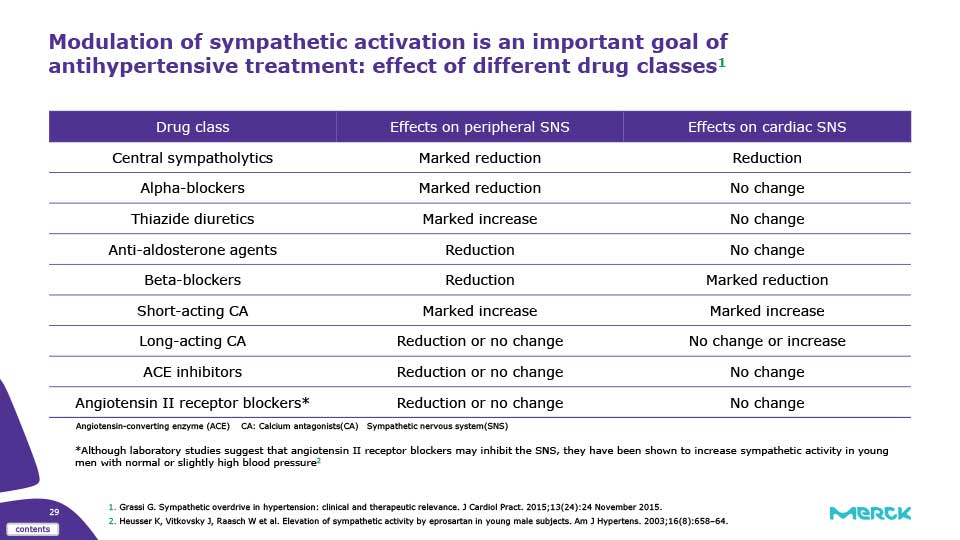
Modulation of sympathetic activation is an important goal of antihypertensive treatment: effect of different drug classes
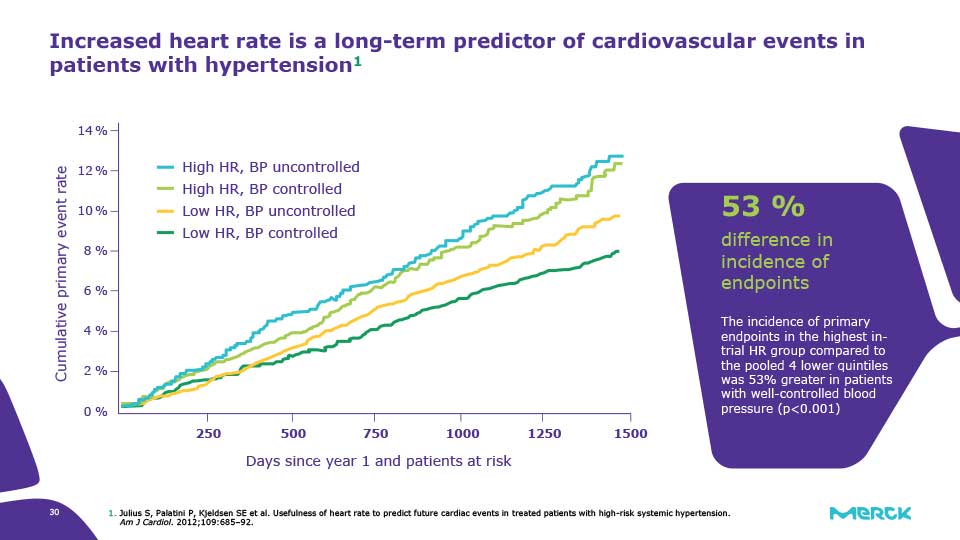
Increased heart rate is a long-term predictor of cardiovascular events in patients with hypertension
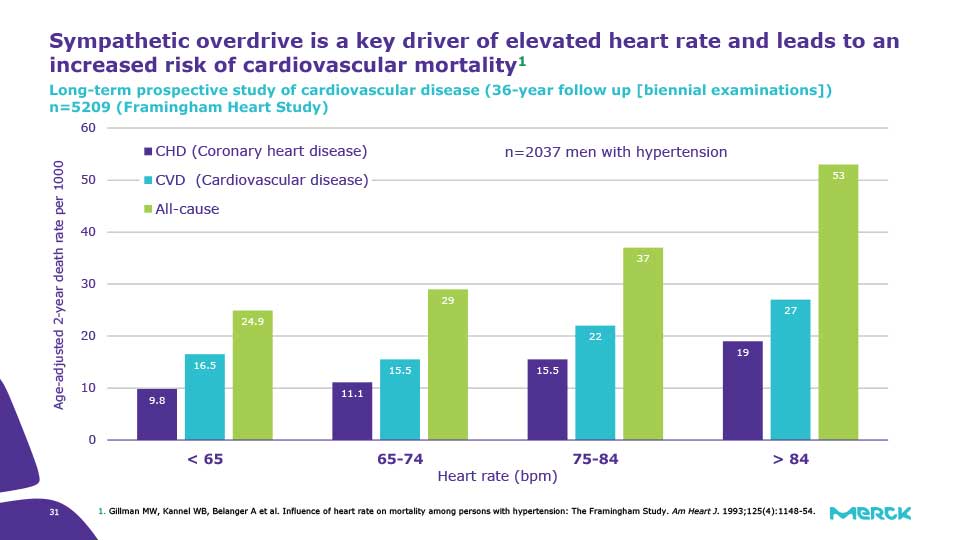
Sympathetic overdrive is a key driver of elevated heart rate and leads to an increased risk of cardiovascular mortality
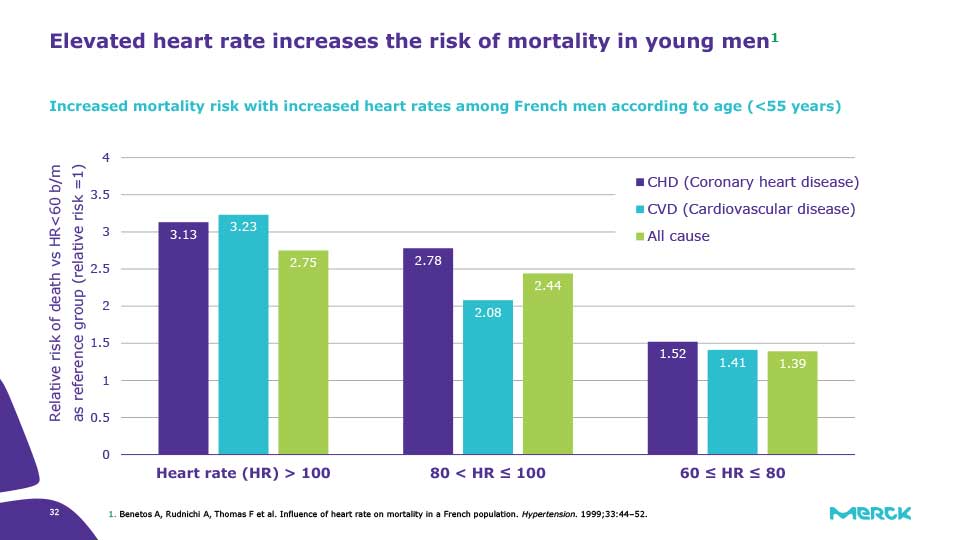
Elevated heart rate increases the risk of mortality in young men
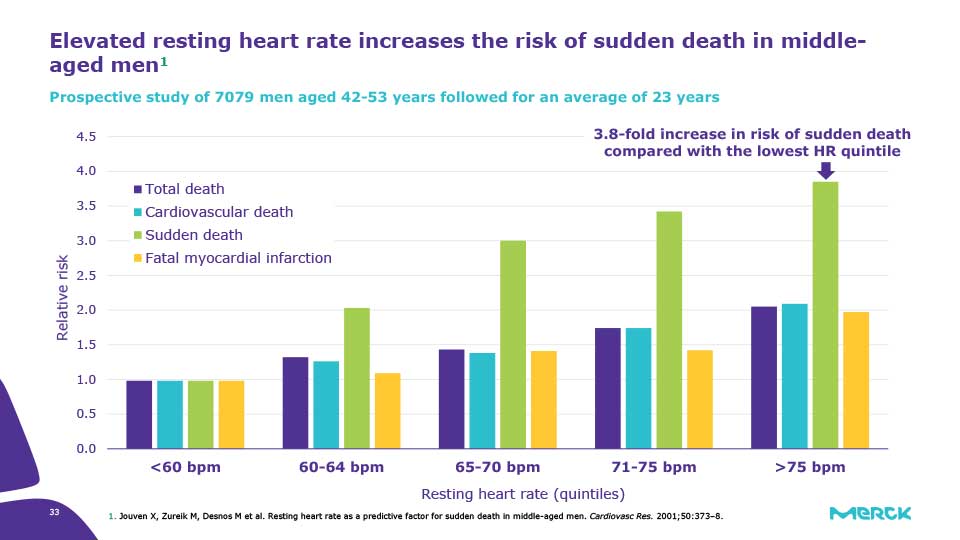
Elevated resting heart rate increases the risk of sudden death in middle-aged men
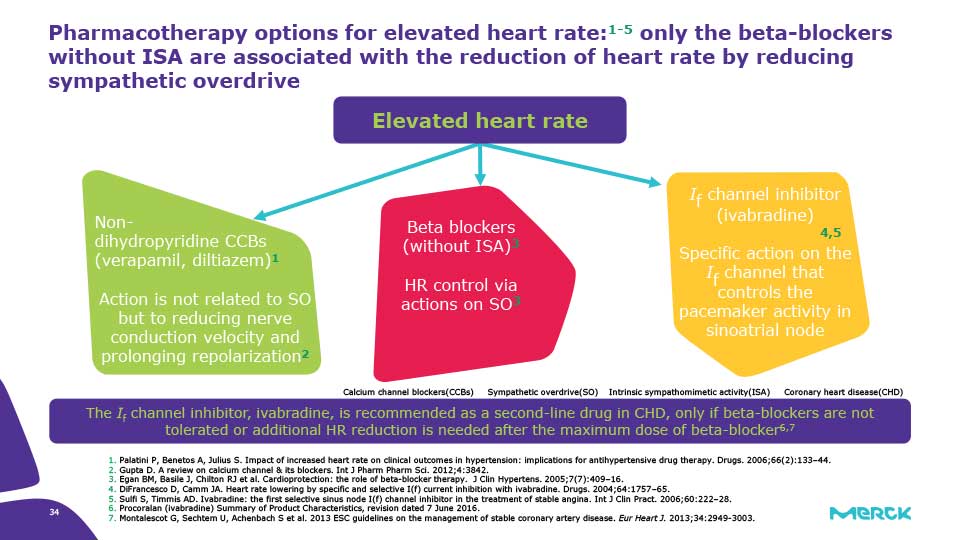
Pharmacotherapy options for elevated heart rate:1-5 only the beta-blockers without ISA are associated with the reduction of heart rate by reducing sympathetic overdrive
Summary of office BP thresholds for treatment
{kind=link}
Drug treatment strategy for hypertension - 1
{kind=link}
Underlying causes of hypertension differ between the young and old – Framingham Heart Study
{kind=link}
Sympathetic overdrive plays a key role in the pathophysiology of cardiovascular disease
{kind=link}
Sympathetic overdrive leads to multiple responses that contribute to heart failure and sudden death
{kind=link}
Modulation of sympathetic activation is an important goal of antihypertensive treatment: effect of different drug classes
{kind=link}
Increased heart rate is a long-term predictor of cardiovascular events in patients with hypertension
{kind=link}
Sympathetic overdrive is a key driver of elevated heart rate and leads to an increased risk of cardiovascular mortality
{kind=link}
Elevated heart rate increases the risk of mortality in young men
{kind=link}
Elevated resting heart rate increases the risk of sudden death in middle-aged men
{kind=link}
Pharmacotherapy options for elevated heart rate:1-5 only the beta-blockers without ISA are associated with the reduction of heart rate by reducing sympathetic overdrive
{kind=link}
+ What should be the BP treatment target range in such a case?
- SBP <140, DBP <80-70
- SBP <130, DBP <80-70
- SBP <120, DBP <80-70
SHOW ANSWER
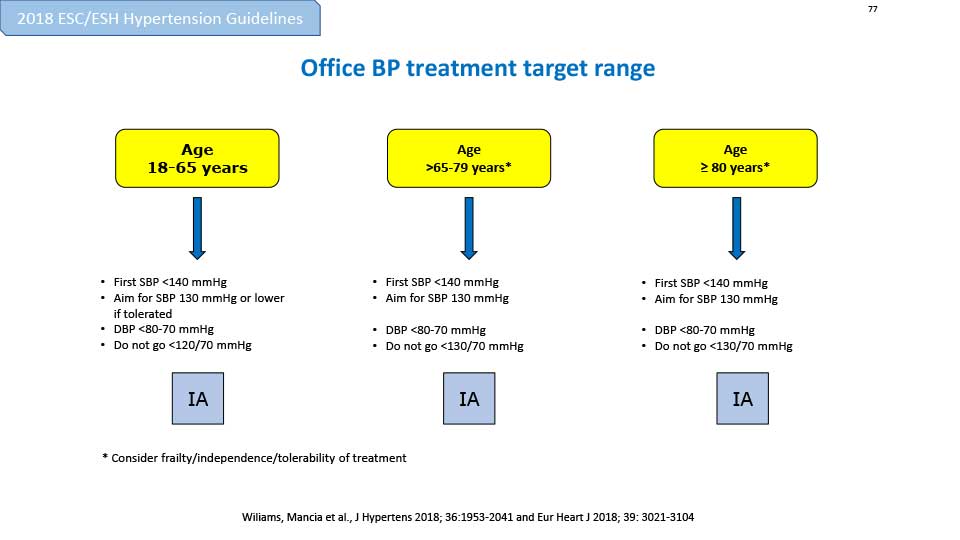{kind=link}
CASE: DIAGNOSIS
- Finally in this case, all secondary causes were excluded
- The diagnosis of hypertension was confirmed with ABPM showing mean diurnal BP ( 146/94) , no orthostatic hypotension a dipping profile.
- This could have been suspected by the profile ( overweight , normal high office BP)
{kind=link}
CASE: TREATMENT
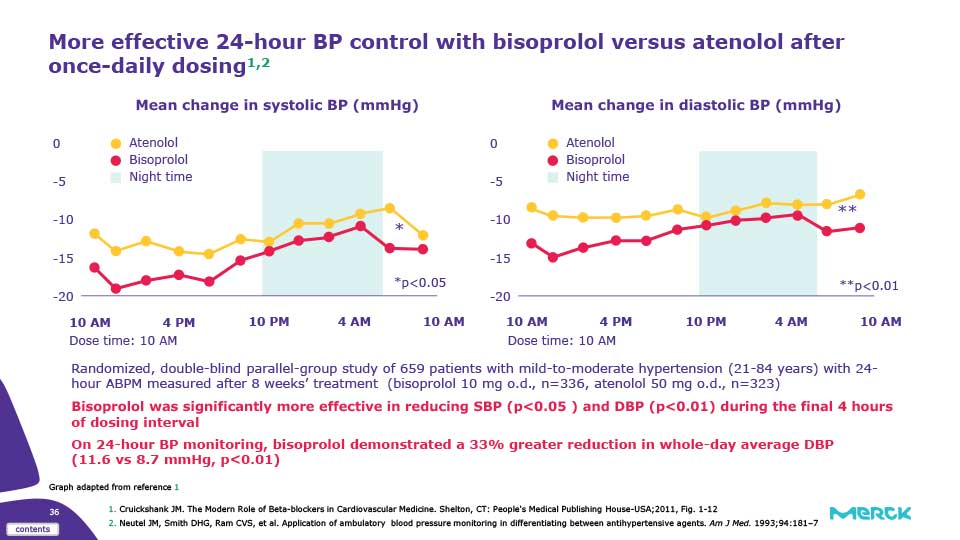
- The patient has been started on atenolol 50 mg o.d.
- He is now feeling better but complains of having some sexual dysfunction.
- He would like to switch to other beta blocker but his friend told him that all medications are the same.
{kind=link}
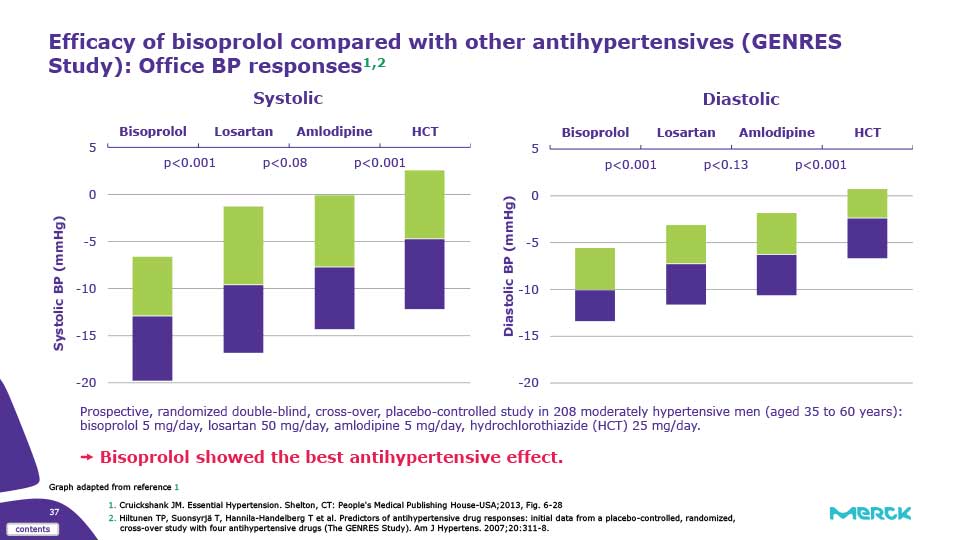
Efficacy of bisoprolol compared with other antihypertensives (GENRES Study): Office BP responses
{kind=link}
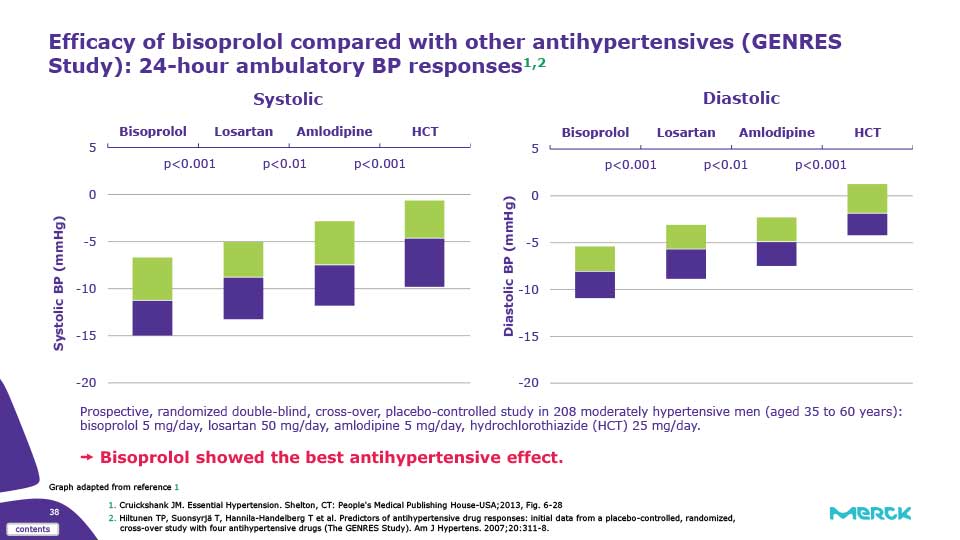
Efficacy of bisoprolol compared with other antihypertensives (GENRES Study): 24-hour ambulatory BP responses
{kind=link}
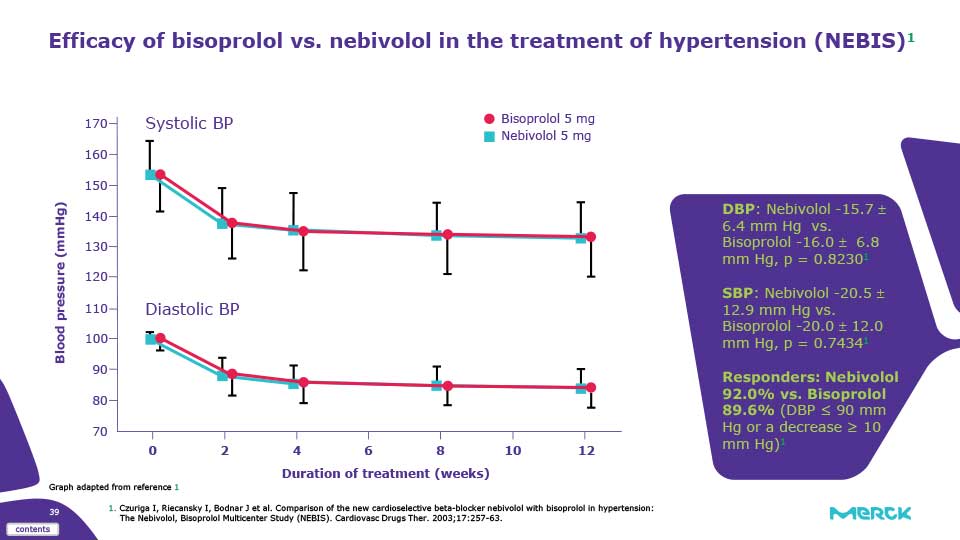
Efficacy of bisoprolol vs. nebivolol in the treatment of hypertension (NEBIS)
{kind=link}
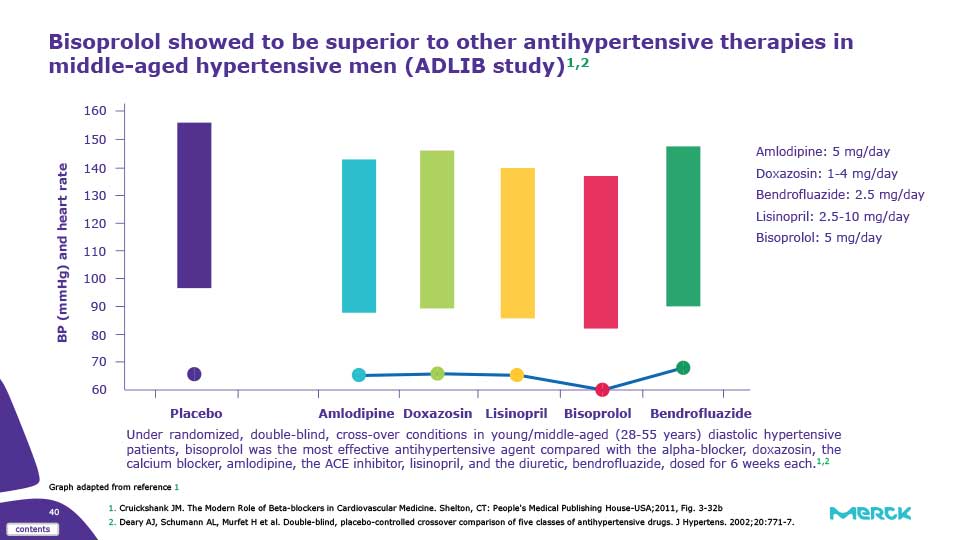
Bisoprolol showed to be superior to other antihypertensive therapies in middle-aged hypertensive men (ADLIB study)
{kind=link}
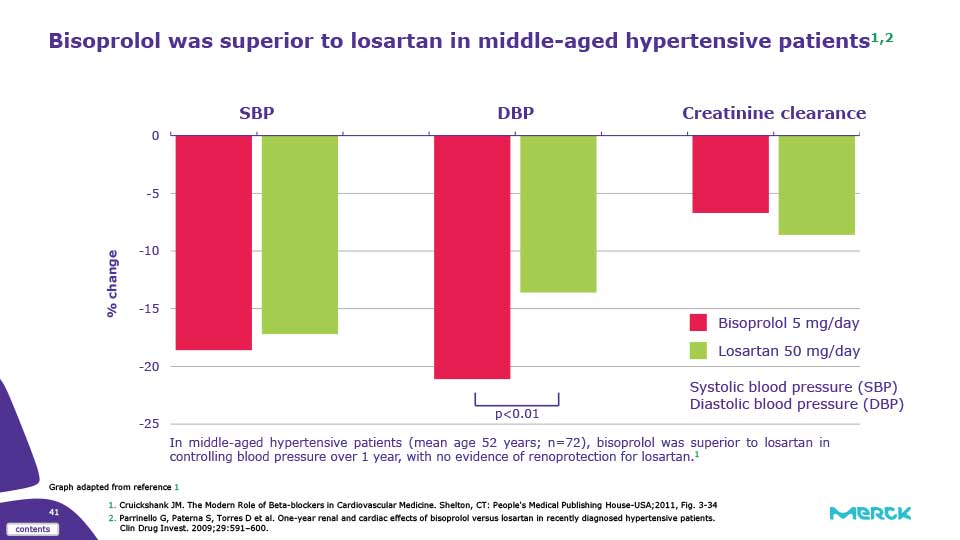
Bisoprolol was superior to losartan in middle-aged hypertensive patients
{kind=link}
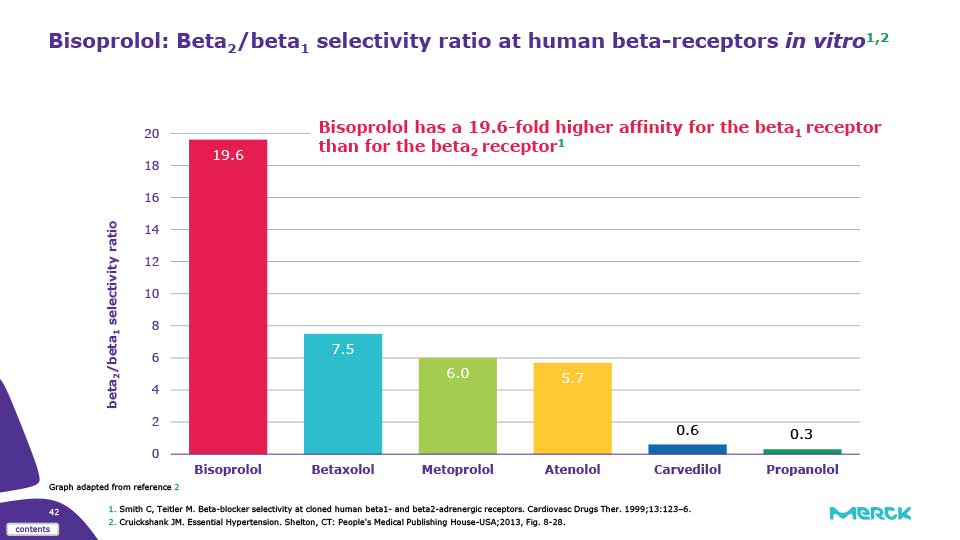
Bisoprolol: Beta2/beta1 selectivity ratio at human beta-receptors in vitro
{kind=link}
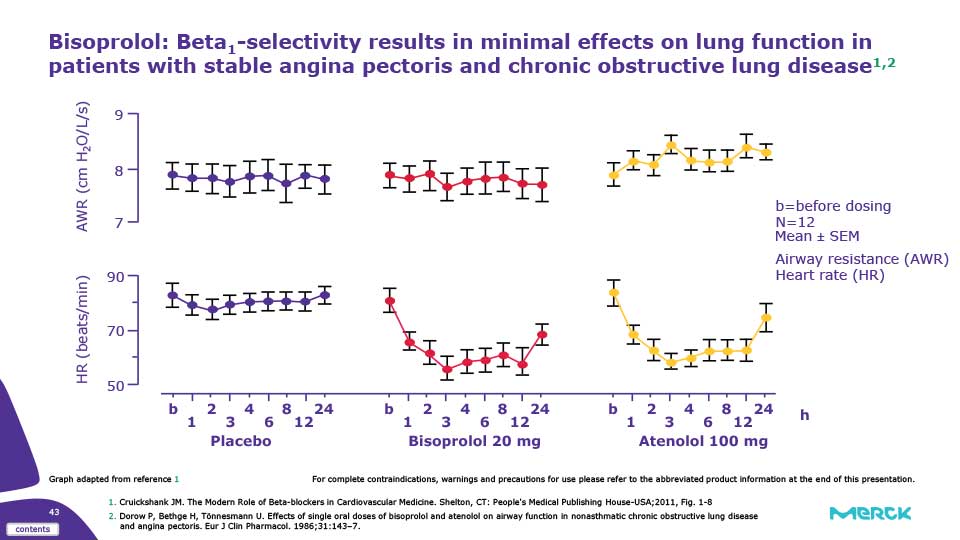
Bisoprolol: Beta1-selectivity results in minimal effects on lung function in patients with stable angina pectoris and chronic obstructive lung disease
{kind=link}
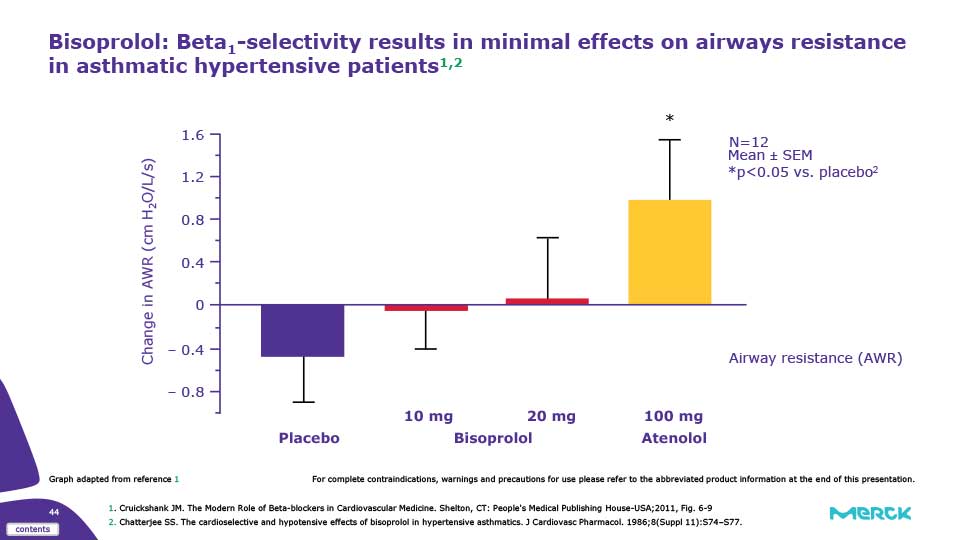
Bisoprolol: Beta1-selectivity results in minimal effects on airways resistance in asthmatic hypertensive patients
{kind=link}
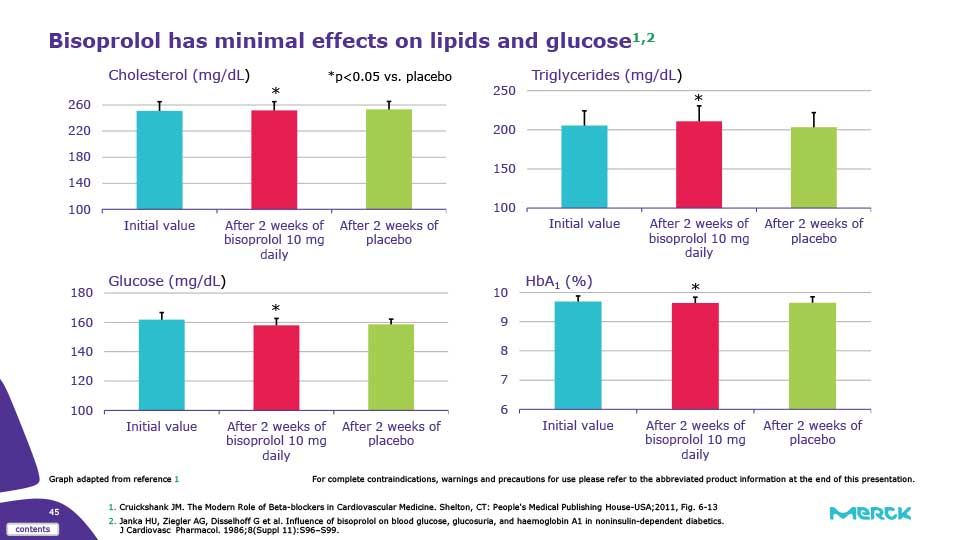
Bisoprolol has minimal effects on lipids and glucose1,2
{kind=link}
WRAP UP
Efficacy
Greater SBP & DBP reduction vs. atenolol1, as well as other antihypertensive agents such as losartan, amlodipine and hydrochlorothiazide2 Better heart rate reduction vs. metoprolol,3 carvedilol and nebivolol4.
β1-Selectivity
Bisoprolol is a third generation beta blocker with a remarkably high beta1-selectivity7.
Safety profile
Minimal effects on blood glucose*, and lipids8-10, as well as lung function**8,11, peripheral circulation12-15, and male sexual function16
Consistent pharmacokinetic profile with a balanced renal clearance and hepatic metabolism17-19.