
HTN, obese male patient, elevated heart rate, insulin resistance, OSA and SO
41 years old.
WATCH WEBINAR
 Case Presentation
Case Presentation
 Questions
Questions
 Case: Treatment
Case: Treatment
 Wrap Up
Wrap Up
CASE PRESENTATION
- The patient is now 41-years-old, obese, and is admitted at the hospital due to shortness of breath and arterial hypertension.
He was diagnosed with arterial hypertension when he was 22 years.
In the ward, he presented with intense dyspnea and arterial hypertension with BP levels of 190 /110 mm Hg.
His adherence to treatment was irregular.
He started to present episodes of intense snoring during sleep and a sensation of suffocation upon awakening.
The patient admits of being obese and that his weight has progressively increased since the age of 28 years.
-
Physical examination
weight=112 kg, height
body mass index was 31
pulse of 101 bpm, BP 200/110 mm Hg -
Pulmonary assessment found
crackles auscultation did not disclose any extra heart sounds abdomen was large; presented an "abdominal apron", without visceromegaly; slight lower-limb edema and decreased pulse in the lower limbs -
Chest X-ray showed
normal heart size -
Electrocardiogram (ECG) (March 7, 2001) showed
sinus rhythm, heart rate of 99 bpm, PR interval of 172 ms, QRS duration of 96 ms, QT interval of 372 ms, a QRS axis shifted (-300), initial notch with QS III wave and aVF, nonprogressive R wave from V1 to V3 and electrical left ventricular hypertrophy -
Echocardiogram showed
septum and posterior wall thickness of 14 mm, aortic diameter of 32 mm, left atrial diameter of 52 mm, left ventricular (LV) diastolic diameter of 47 mm, with ejection fraction of 53%, due to accentuated diffuse hypokinesis
QUESTIONS
+ According to you, what are the causes of secondary HTN in middle aged patients?
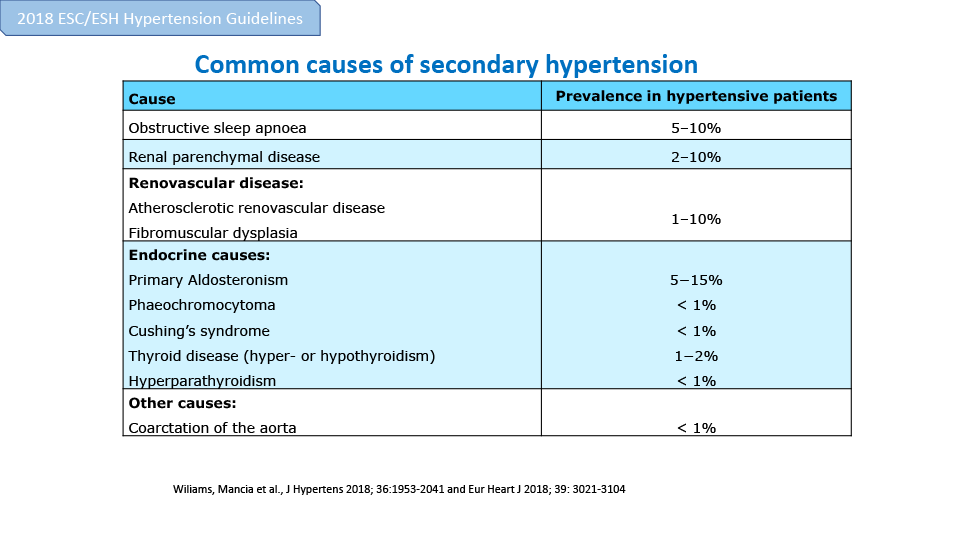
- Primary aldosteronism
- Obstructive sleep apnea
- Cushing’s syndrome
- Coarctation of the aorta
- Phaeochromocytoma
- Monogenic disorders
- Renal parenchymal disease
- Atherosclerotic renovascular disease
- Thyroid disease
Obstructive sleep apnea
Cushing’s syndrome
Phaeochromocytoma
Renal parenchymal disease
Atherosclerotic renovascular disease
Common causes of secondary hypertension
{kind=link}
+ What do you think should be the diagnosis of this case?
- Primary hypertension
- Secondary hypertension
Incidence and typical causes of secondary hypertension according to age
{kind=link}
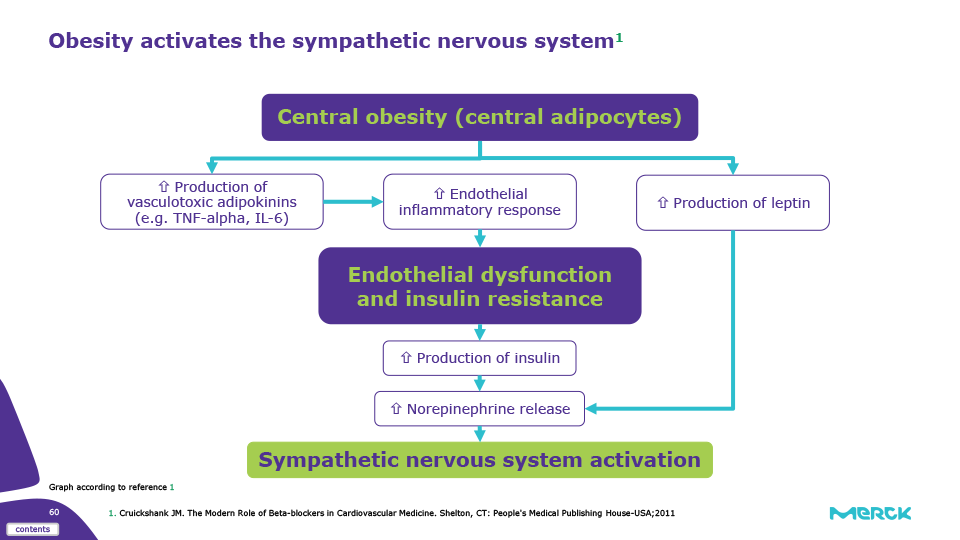
Obesity activates the sympathetic nervous system
{kind=link}
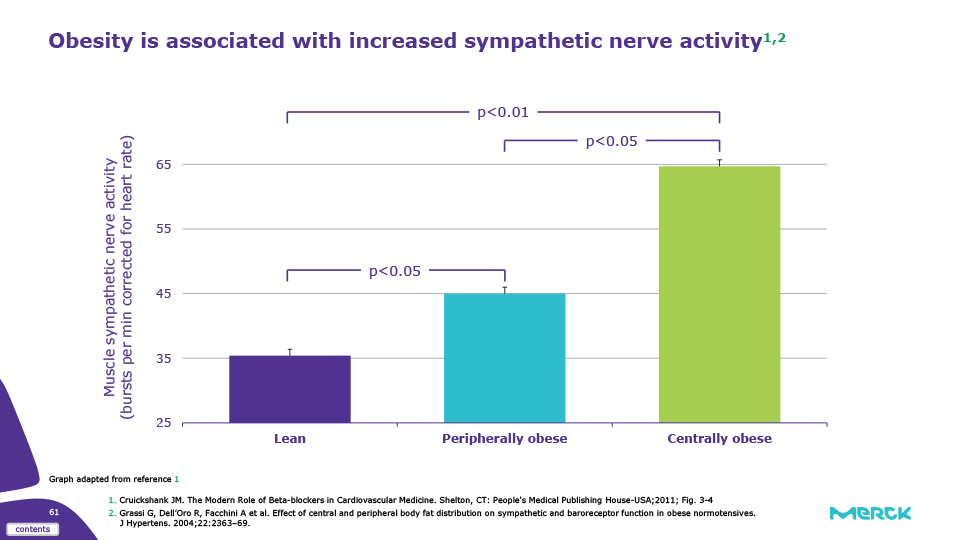
Obesity is associated with increased sympathetic nerve activity
{kind=link}
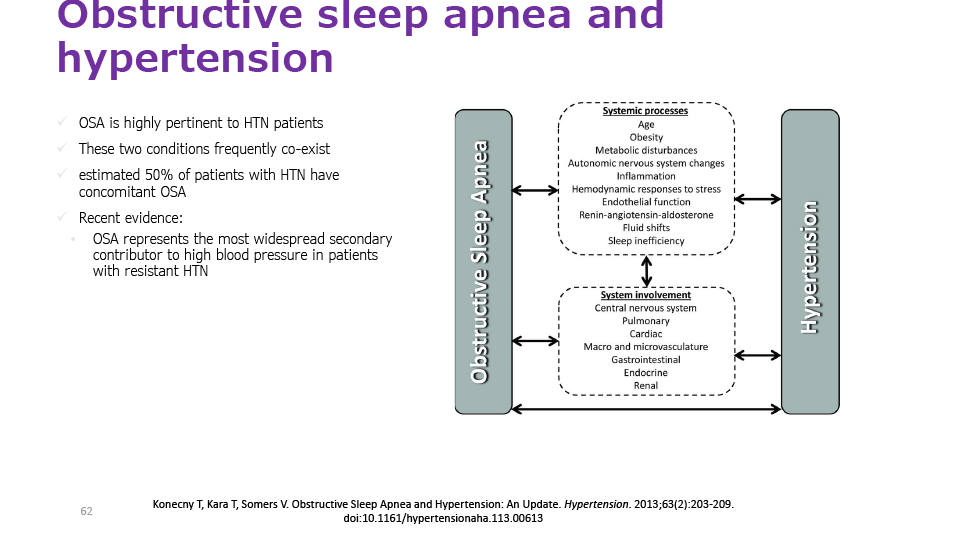
Obstructive sleep apnea and hypertension
{kind=link}
Obstructive sleep apnea and obesity
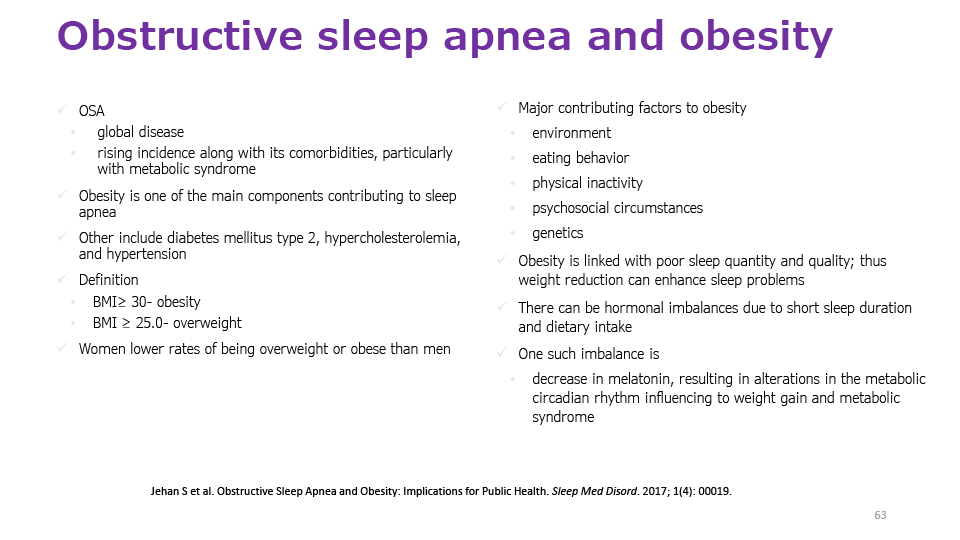{kind=link}
Obstructive sleep apnea and obesity - 2
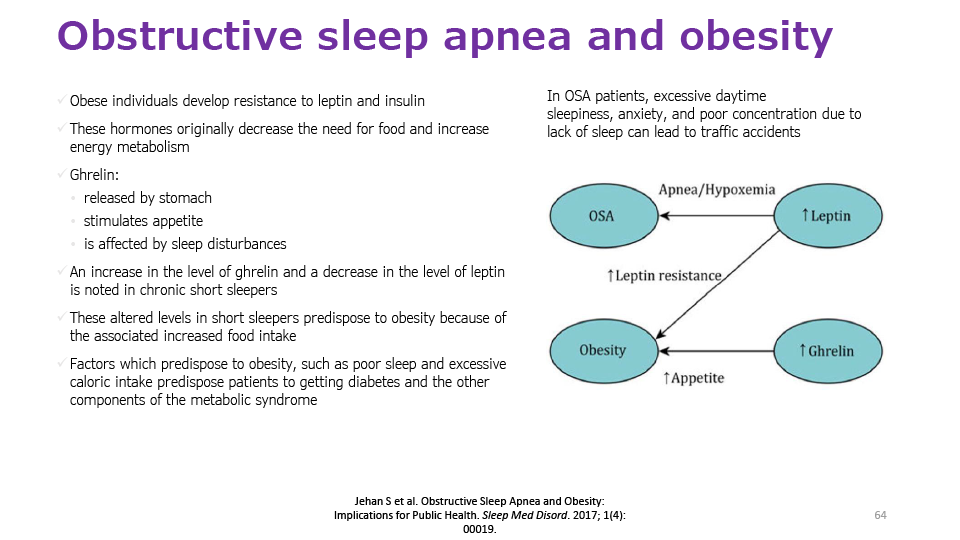{kind=link}
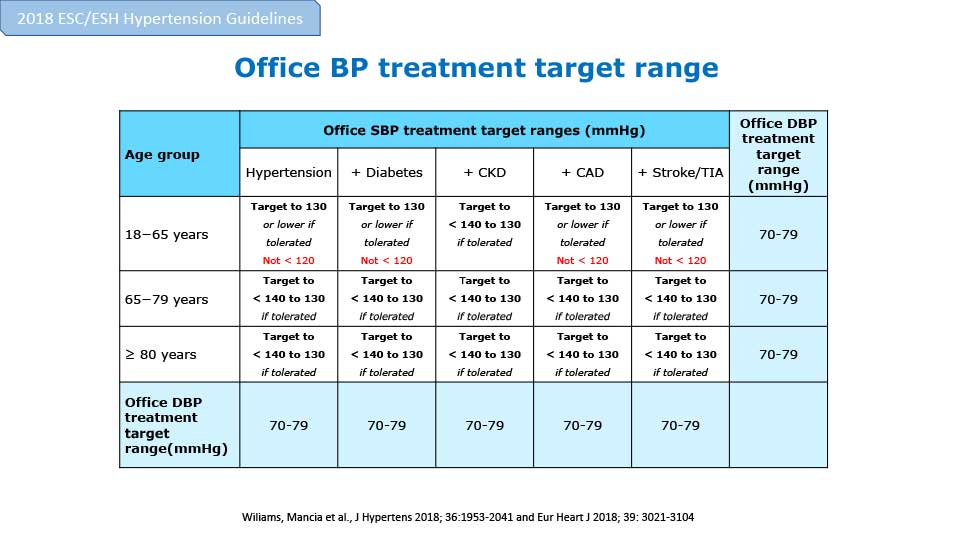
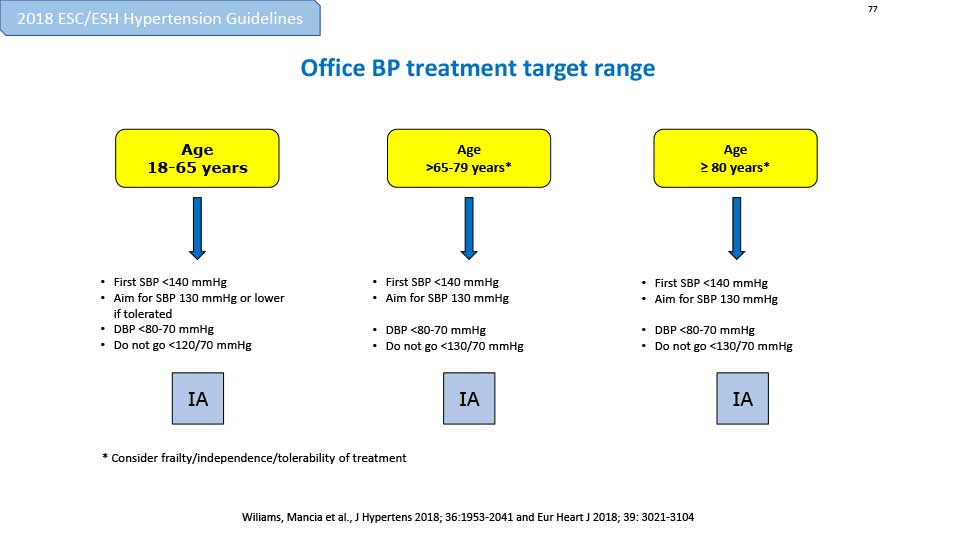
+ What should be the BP threshold for treatment in such a case?
- SBP≥140, DBP≥90
- SBP≥90, DBP≥90
- SBP≥140, DBP=90
{kind=link}
{kind=link}
CASE: TREATMENT
The patient was medicated with 40 mg of furosemide.
Bisoprolol was maintained.
The patient was also recommended a low-salt, low-calorie diet for his weight OR The patient was also recommended a low-salt, low-calorie diet for his obesity problem.
His adherence to treatment, together with dietary changes, resulted in weight loss of 28 kg symptom improvement.
BP reduction to 150/90 mmHg.
OSA treatment with Positive Pressure further reduced office BP to 134/82 and HBPM confirmed that the patient was controlled.
The patient’s heart rate is still 98 bpm, with complaints of palpitation
{kind=link}
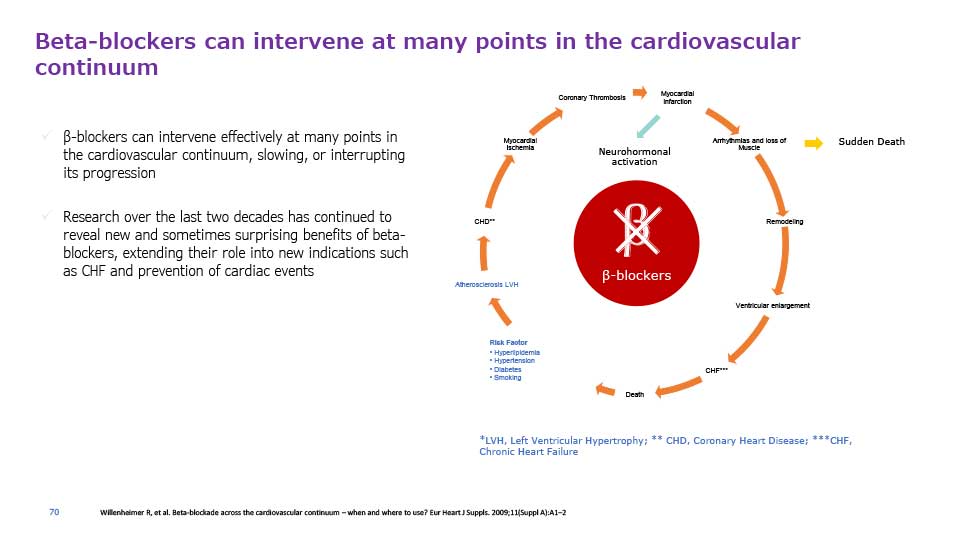
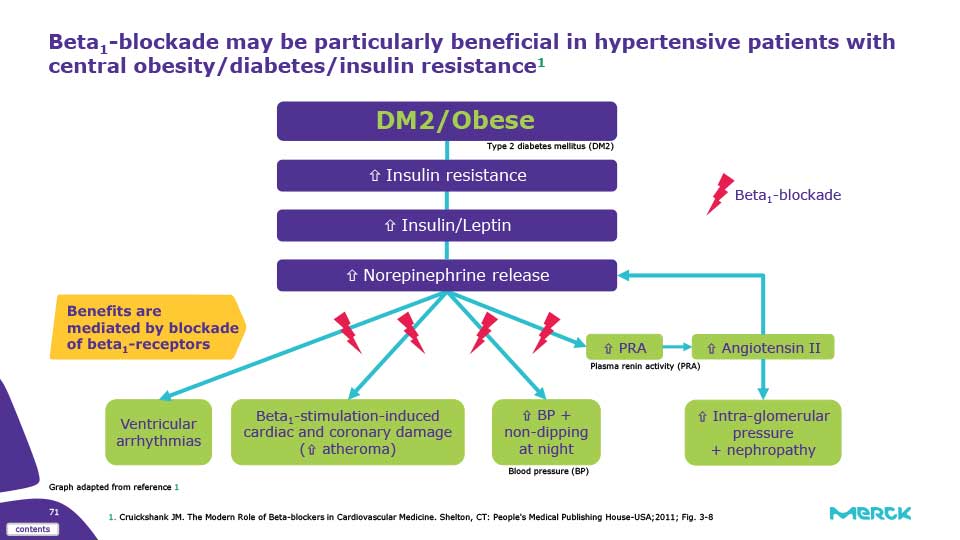
Beta1-blockade may be particularly beneficial in hypertensive patients with central obesity/diabetes/insulin resistance
{kind=link}
Do you think bariatric surgery will have an impact on the patient’s BP and cardiac complication?
Hypertension is associated with obesity, and weight loss remains a first-line therapy in treating HTN
Lifestyle modification and pharmacologic: meet with treatment failure
Bariatric surgery: most successful approach to sustained weight loss
Aim: A randomized, single-center, nonblinded trial was conducted by Schiavon C et al to assess the impact of bariatric surgery in individuals with obesity and HTN
Study results:
Inclusion: 100 patients (70% female, mean age 43.8±9.2 years, mean BMI 36.9±2.7 kg/m2); 96% completed follow-up
Reduction of ≥30% of the total number of antihypertensive medications, maintaining controlled BP in 83.7% patients from the gastric bypass group compared to 12.8% from the control group with a rate ratio of 6.6
Remission of HTN was seen in 51% and 45.8% patients randomized to gastric bypass, considering office and 24-hour ambulatory blood pressure monitoring, respectively, whereas no patient submitted to medical therapy was free of antihypertensive drugs at 12 months
Post hoc analysis for the primary end point considering the SPRINT (Systolic Blood Pressure Intervention Trial) target
rate ratio of 3.8. 11 patients from the gastric bypass group and none in the control group were able to achieve SPRINT levels without antihypertensives
Waist circumference, BMI, low-density lipoprotein cholesterol, triglycerides, fasting plasma glucose, glycohemoglobin, high-sensitivity C-reactive protein, and 10-year Framingham risk score lower in the gastric bypass than in the control group
Study concluded that bariatric surgery represents an effective strategy for blood pressure control in a broad population of patients with obesity and hypertension
WRAP UP
Objective
The reduction in the sympathetic cardiovascular drive may:
Prevent the HR elevation induced by SO
Prevent BP rise induced by OSA related sympathoexcitation
Neutralize metabolic effect of insulin resistance mediated by SO
Prevent progression into the CV continuum driven by SO
Efficacy
Greater SBP & DBP reduction with bisoprolol vs. atenolol1, as well as other antihypertensive agents such as losartan, amlodipine and hydrochlorothiazide2
Better heart rate reduction vs. metoprolol,3 carvedilol and nebivolol4
β1-Selectivity
Bisoprolol is a third generation beta blocker with a remarkably high beta1-selectivity7
Safety profile
Minimal effects on blood glucose*, and lipids8-10, as well as lung function**8,11, peripheral circulation12-15, and male sexual function16
Consistent pharmacokinetic profile with a balanced renal clearance and hepatic metabolism17-19