
 Case Presentation
Case Presentation
 Medical History
Medical History
 Questions
Questions
 Wrap Up
Wrap Up
CASE PRESENTATION
- The patient is now 62 year-old, admitted to the hospital with progressive dyspnea on exertion, bilateral ankle edema, an elevated jugular venous pressure, and bibasilar pulmonary crackles
His blood pressure is 162/88 mm Hg, heart rate 86 beats per minute, sinus rhythm; he has a third heart sound and a 2/6 ejection systolic murmur
Serum electrolyte concentrations are normal
His nt pro BNP is close to 9231 pg/ml
The chest radiograph shows moderate cardiomegaly and moderate-to-severe pulmonary venous congestion
An echocardiogram shows increased left ventricular and left atrial lumen diameters, mild mitral regurgitation, mild aortic valve calcification, and an ejection fraction of 32%
MEDICAL HISTORY
- Three years back, he was been discharged from the hospital on bisoprolol 5 mg per day, ramipril 5 mg per day, furosemide 60 mg per day, sublingual nitroglycerin when necessary, and aspirin 100 mg per day, and a statin
His blood pressure on discharge is 128/76 mm Hg and he is hemodynamically stable, with no evidence of left ventricular decompensation. Heart rate 67 bpm >
The patient was followed up every 3 months and was doing well
QUESTIONS
+ How should the case of HTN and heart failure be treated?
- ACEi or ARB + CCB or diuretic
- ACEi or ARB + beta-blocker or CCB or CCB + diuretic or beta-blocker or beta-blocker + diuretic
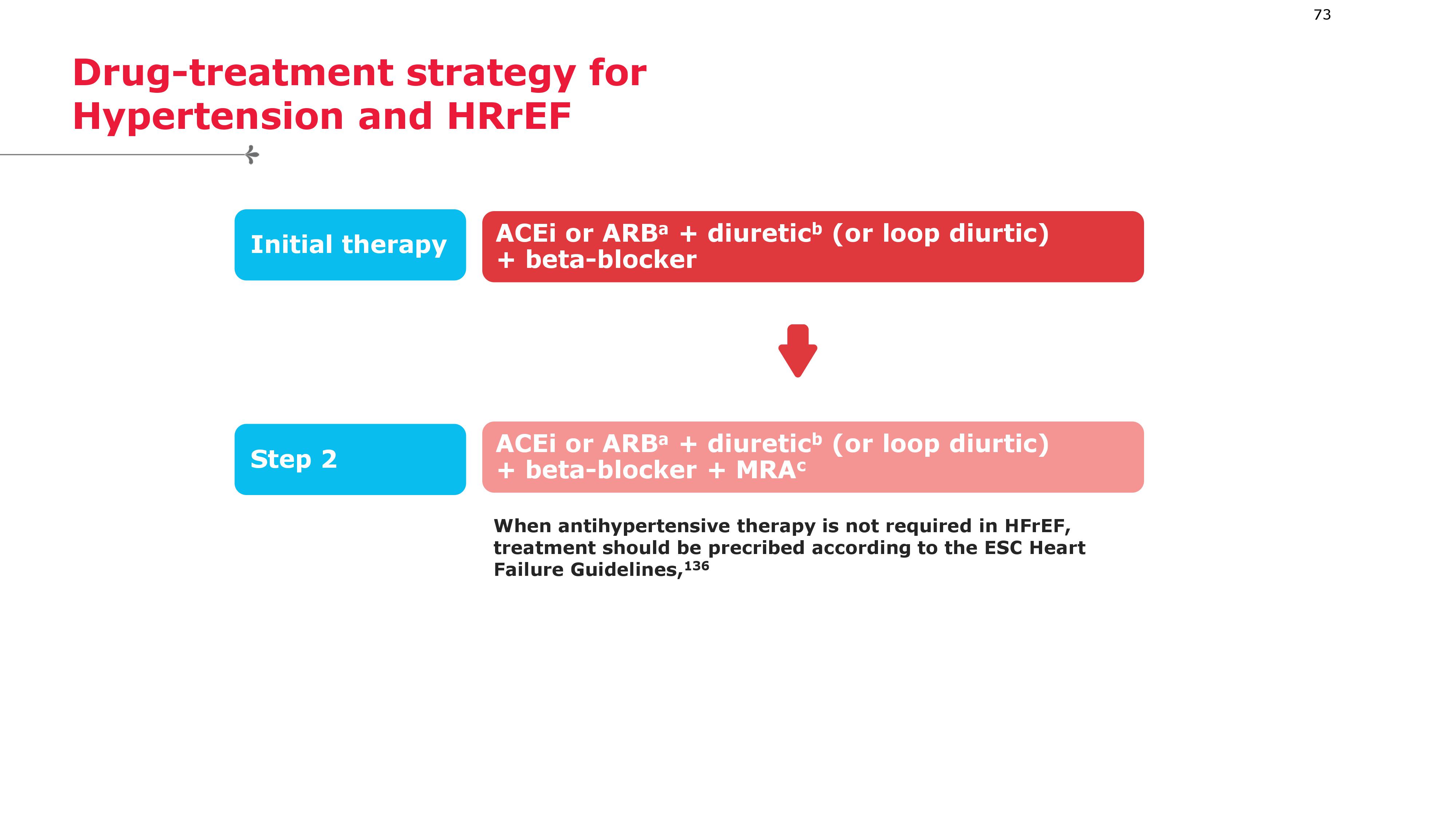
- ACEi or ARB + diuretic (or loop diuretic) + beta-blocker
- ACEi or ARB + beta-blocker or non-DHP CCB, or beta blocker + CCB
Evidence
Drug treatment strategy for hypertension and heart failure with reduced ejection fraction.
Do not use non-dihydropyridine
CCBs (e.g. verapamil or diltiazem). ACEi = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; CCB = calcium channel
blocker; ESC = European Society of Cardiology; HFrEF = heart failure with reduced ejection fraction;MRA = mineralocorticoid receptor antagonist.
a Consider an angiotensin receptor/neprilysin inhibitor instead of ACEi or ARB per ESC Heart Failure Guidelines.
b Diuretic refers to thiazide/thiazide-like diuretic. Consider a loop diuretic as an alternative in patients with oedema.
c MRA (spironolactone or eplerenone).
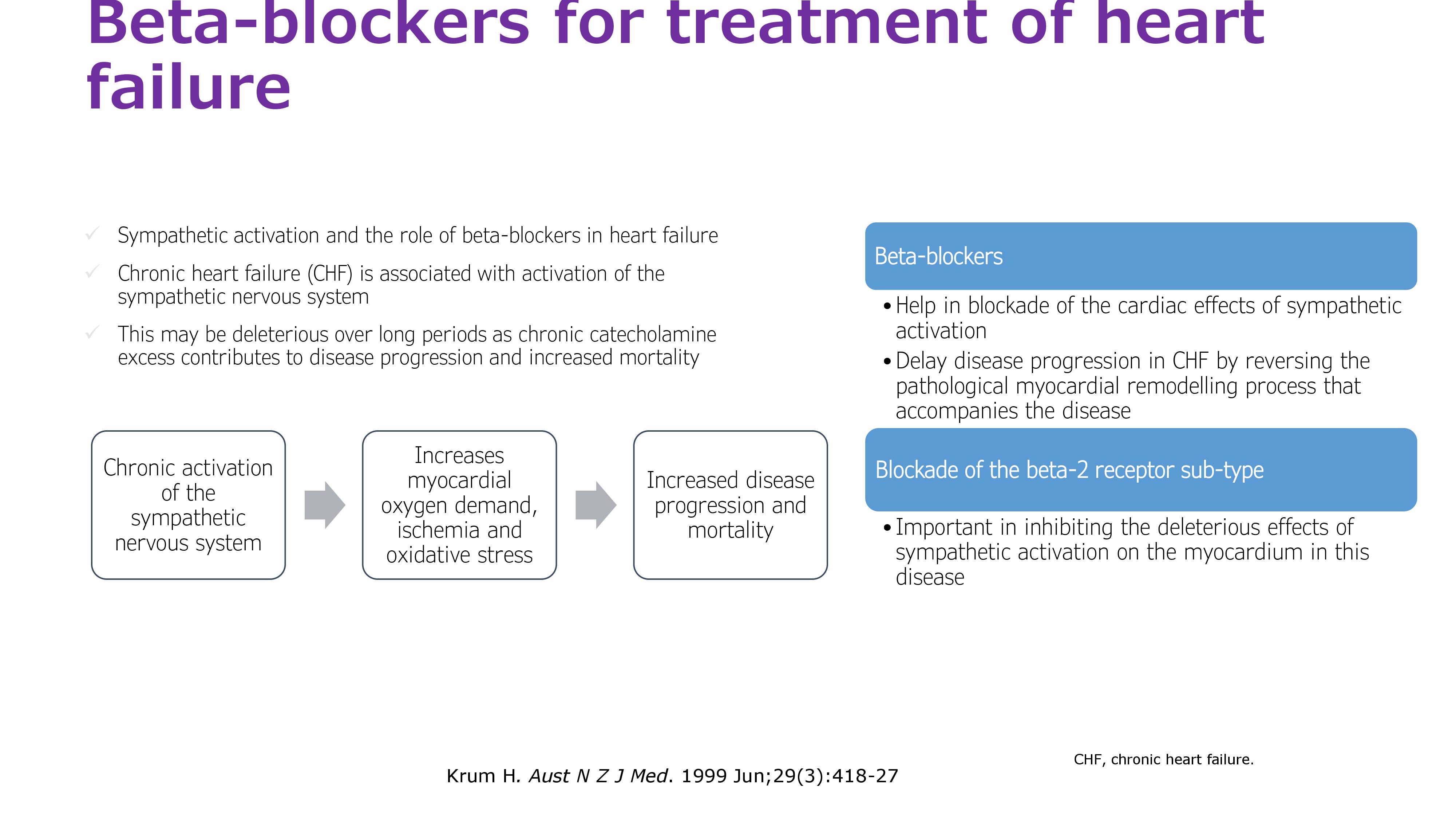
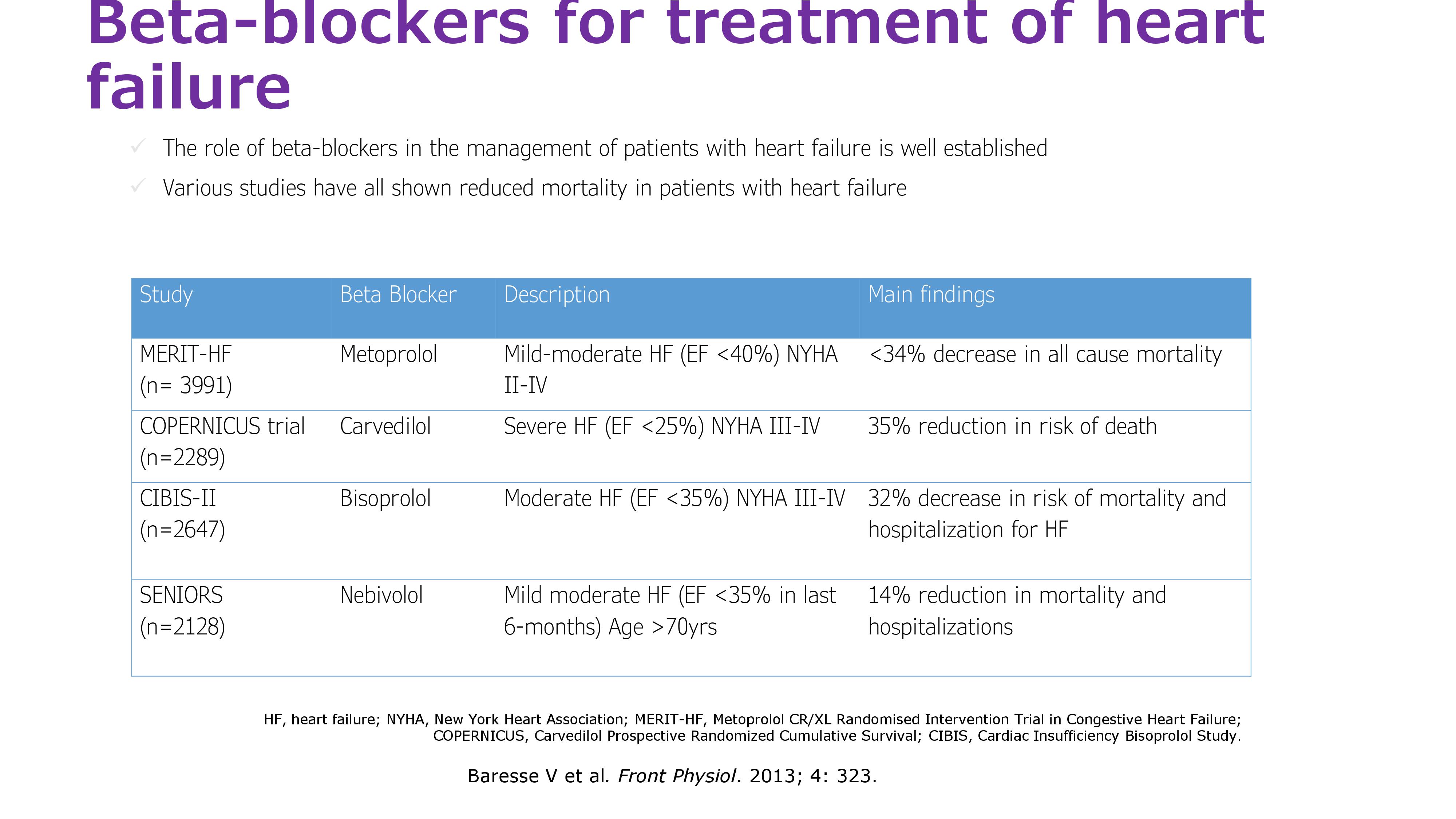
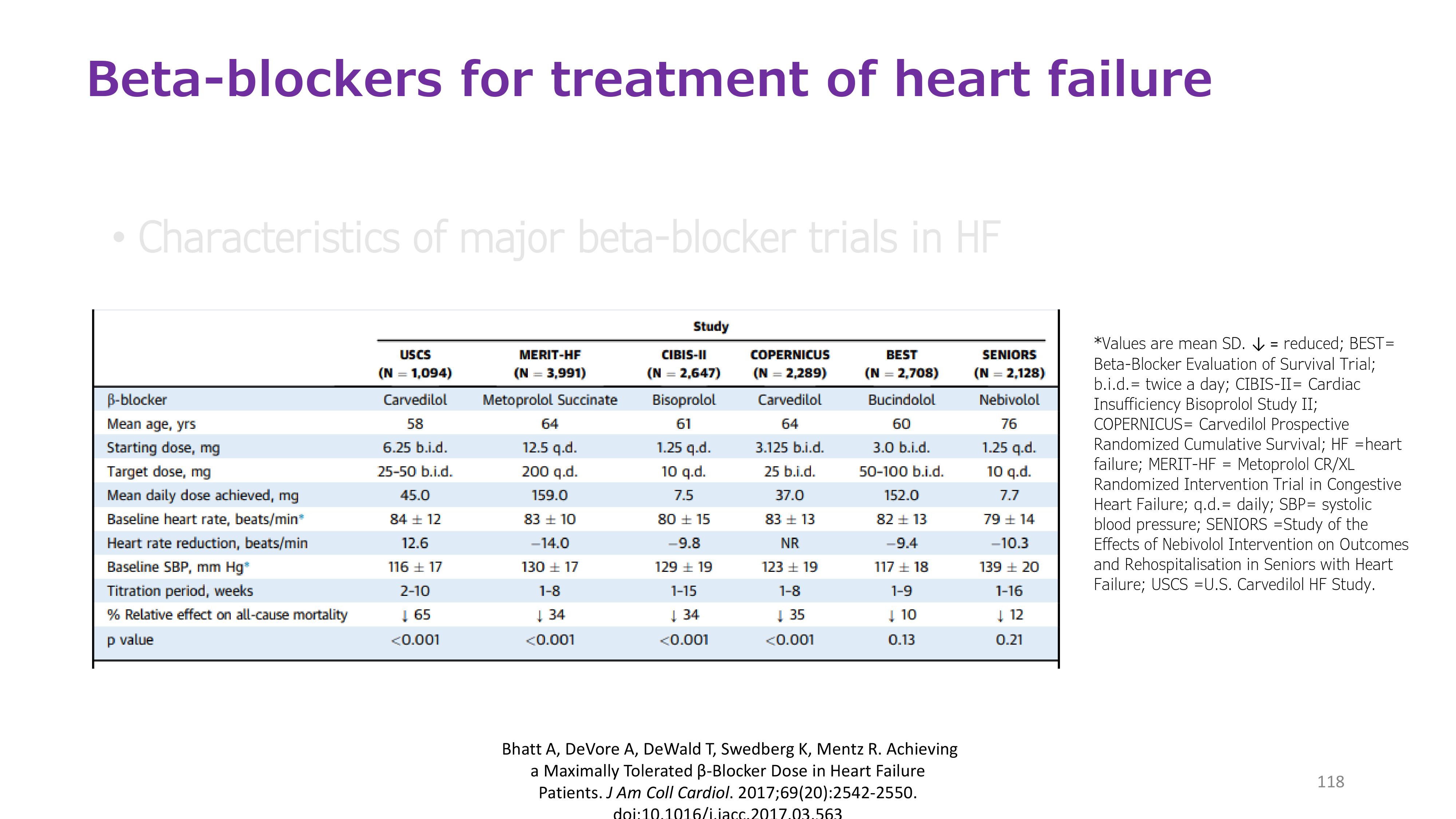
+ Do you think Beta blockers are effective in patients heart failure with reduced ejection fraction (HFrEF)?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
+ What is the BP goal in patients with heart failure?
Evidence
According to the 2017 ACC/AHA/HFSA heart failure guideline
In patients at increased risk, stage A HF, the optimal blood pressure in those with hypertension should be less than 130/80 mm Hg
Patients with HFrEF and hypertension should be prescribed GDMT titrated to attain systolic blood pressure less than 130 mm Hg
Patients with HFpEF and persistent hypertension after management of volume overload should be prescribed GDMT titrated to attain systolic blood pressure less than 130 mm Hg
{kind=link}
Drug-treatment strategy for Hypertension and HRrEF
{kind=link}
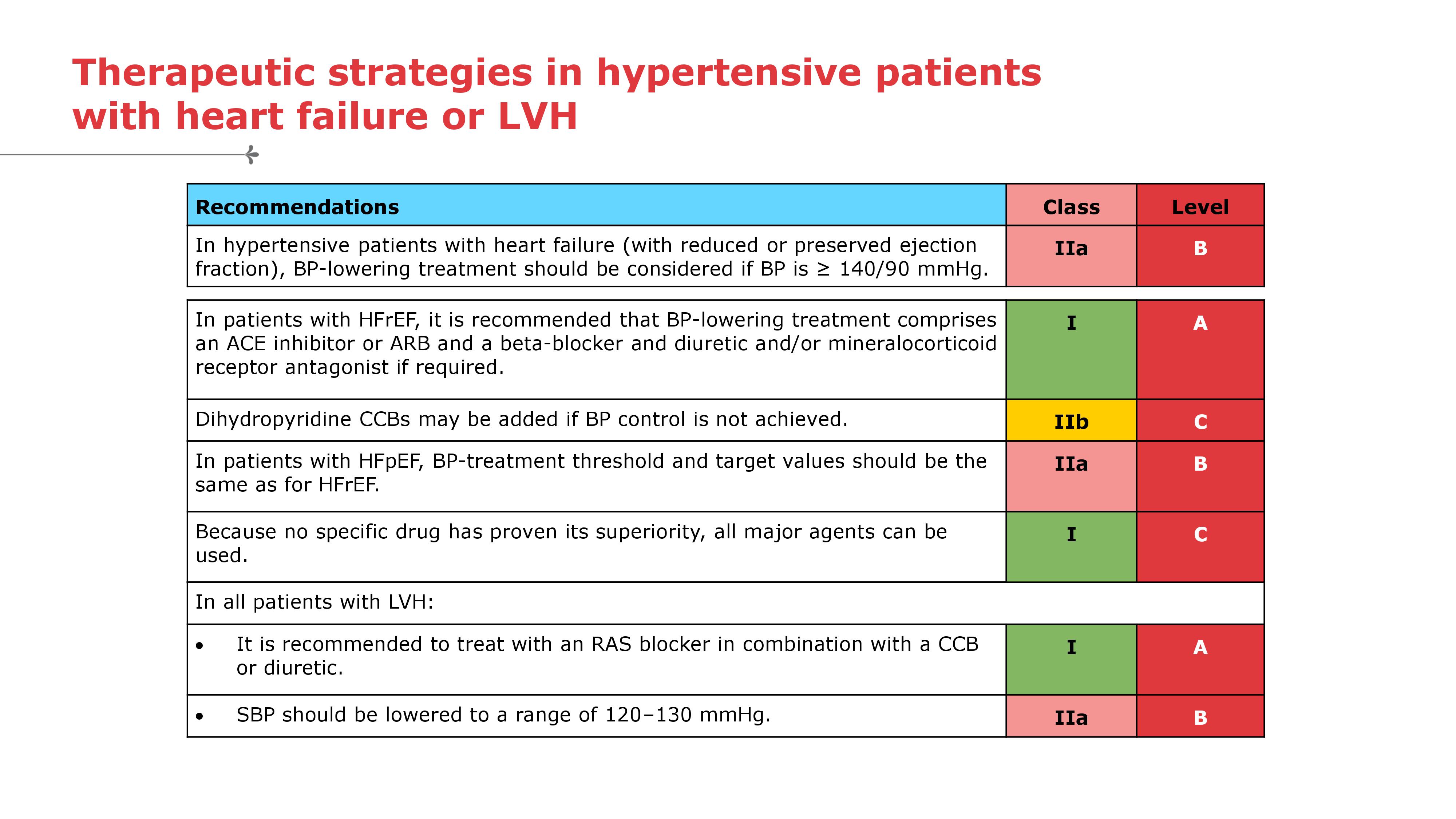
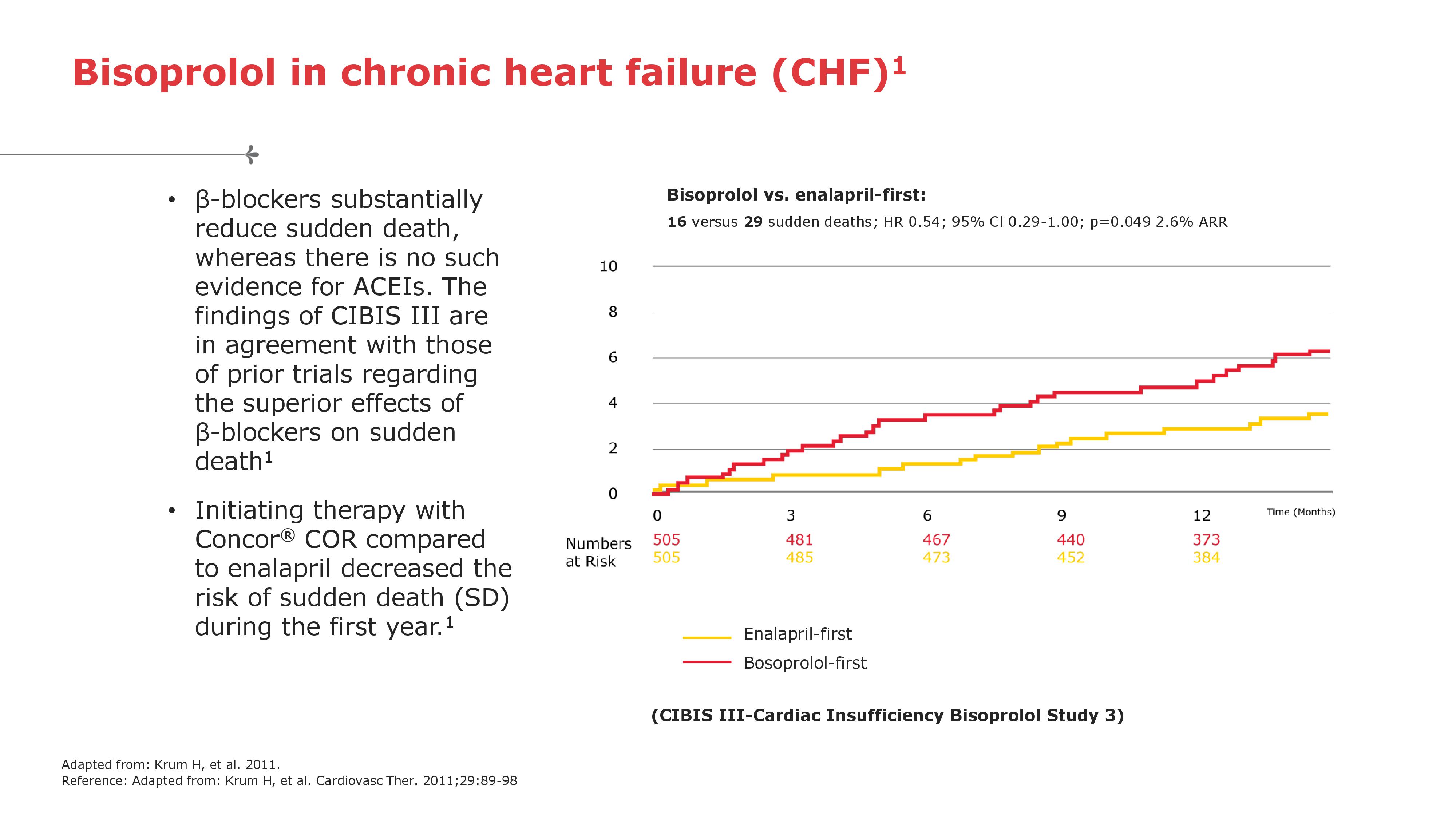
Therapeutic strategies in hypertensive patients with heart failure or LVH Bisoprolol in chronic heart failure (CHF)
{kind=link}
{kind=link}
WRAP UP
The objectives:
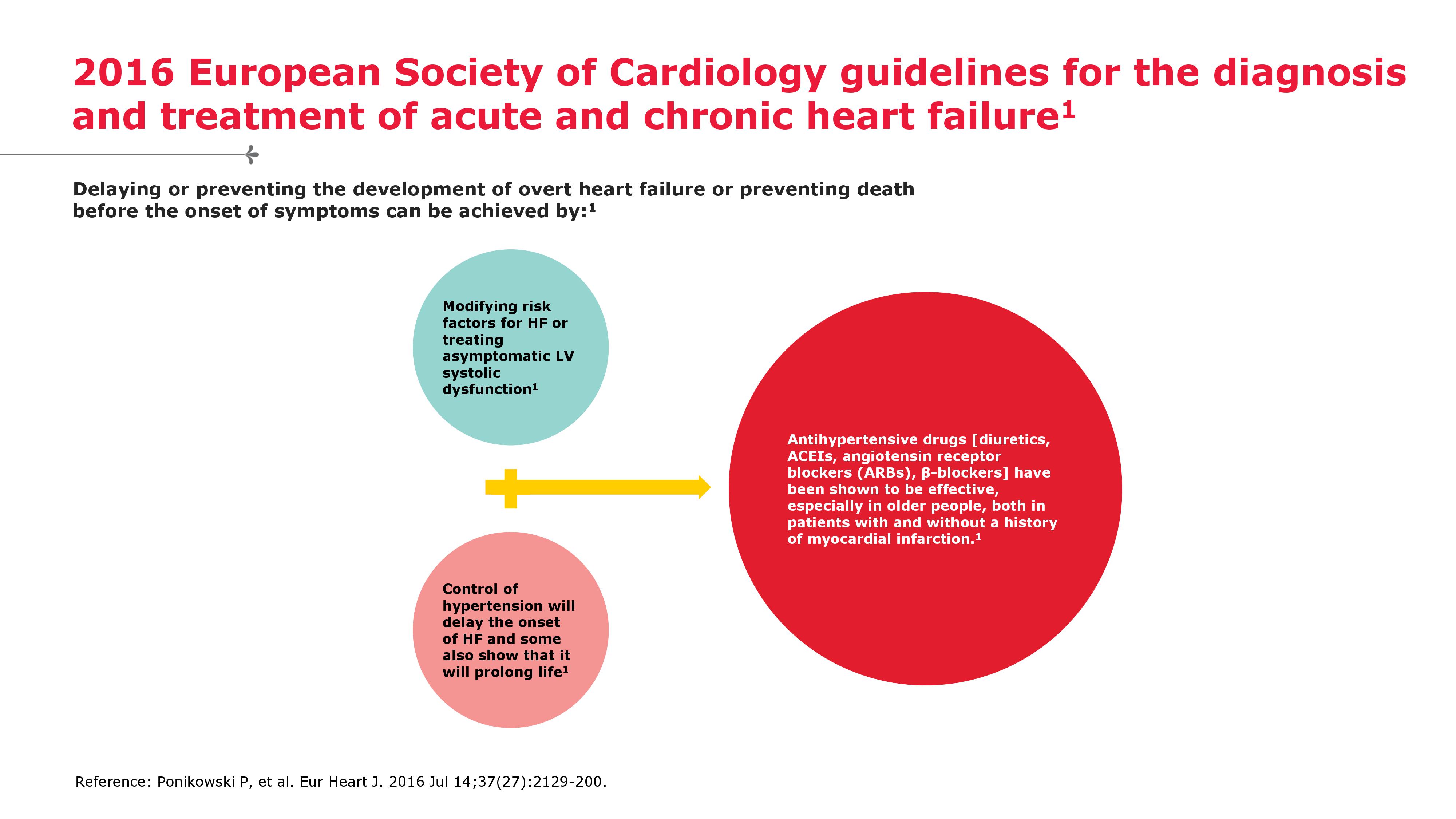
To decrease the likelihood of disease progression (thereby decreasing the risk of death and the need for hospitalization),
To lessen symptoms,
To improve quality of life.
Bisoprolol Efficacy
Reduction of all cause mortality by 34%,
Reduction of sudden death by 44%,
Reduction of hospitalization (all-cause & worsening heart failure) by 20% & 36%.
β1-Selectivity
Bisoprolol is a third generation beta blocker with a remarkably high beta1-selectivity7
Safety profile
Minimal effects on blood glucose*, and lipids8-10, as well as lung function**8,11, peripheral circulation12-15, and male sexual function16
Consistent pharmacokinetic profile with a balanced renal clearance and hepatic metabolism17-19